2016 WHO Criteria
- PB leukocytosis with increased PMNs and precursors (evidence of dysgranulopoiesis)
- Neutrophil precursors (less mature than a band-form) make up ≥10% of leukocytes
- Absence of significant basophilia (<2% or leukocytes)
- No monocytosis (<10% of leukocytes)
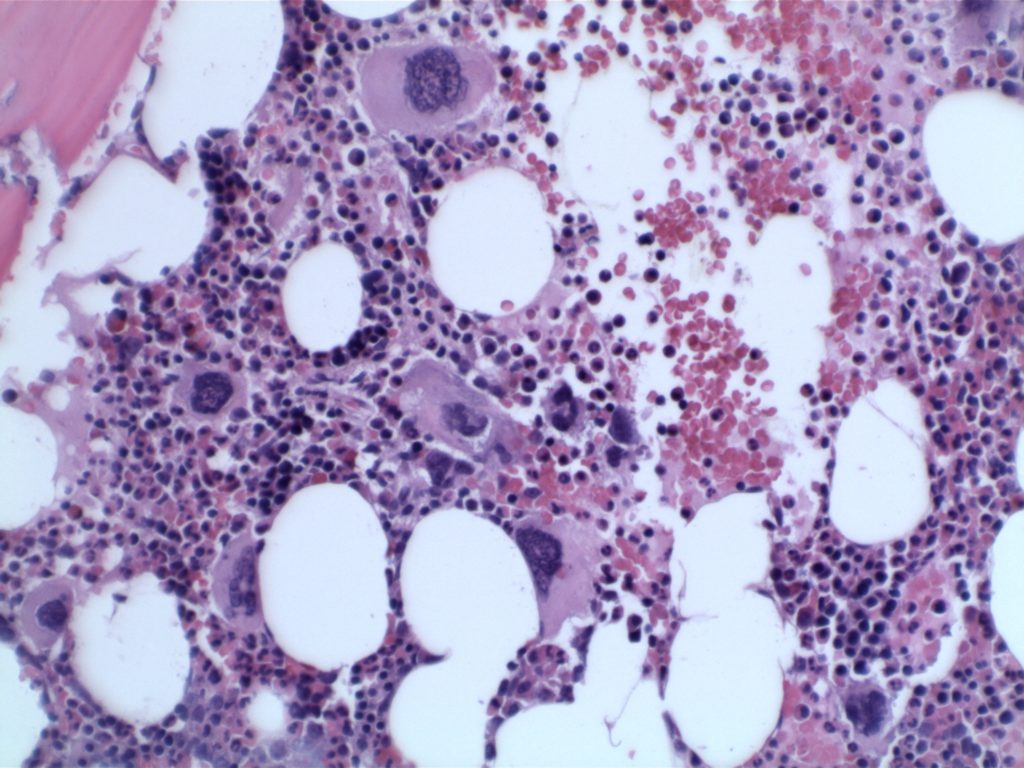
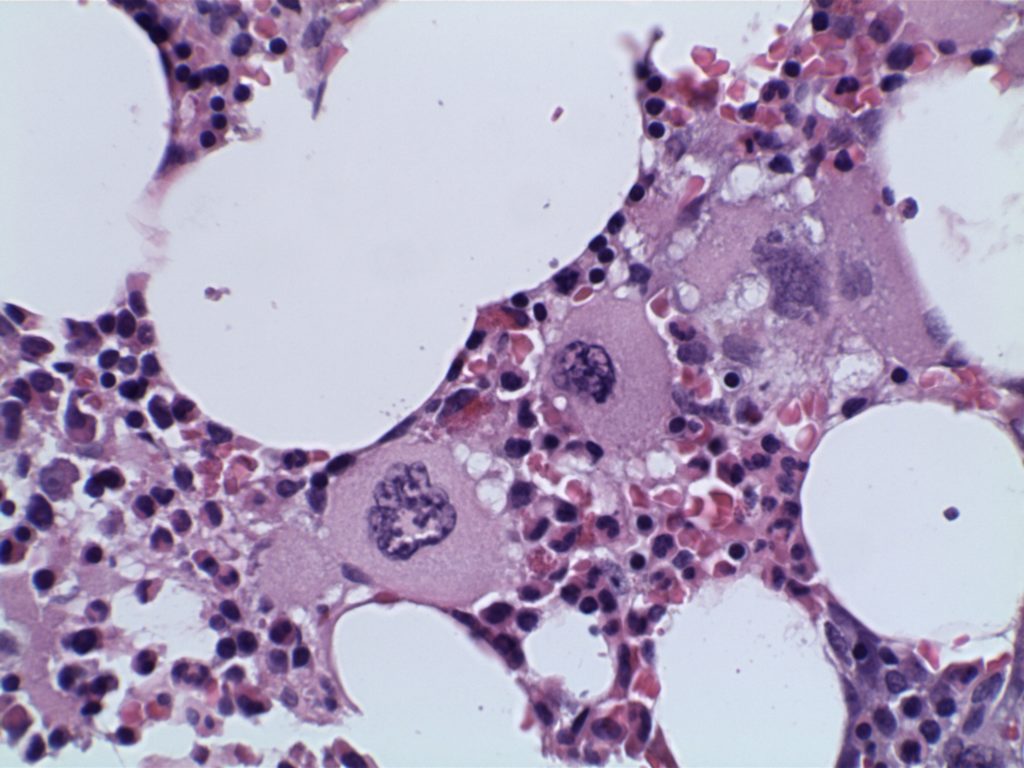
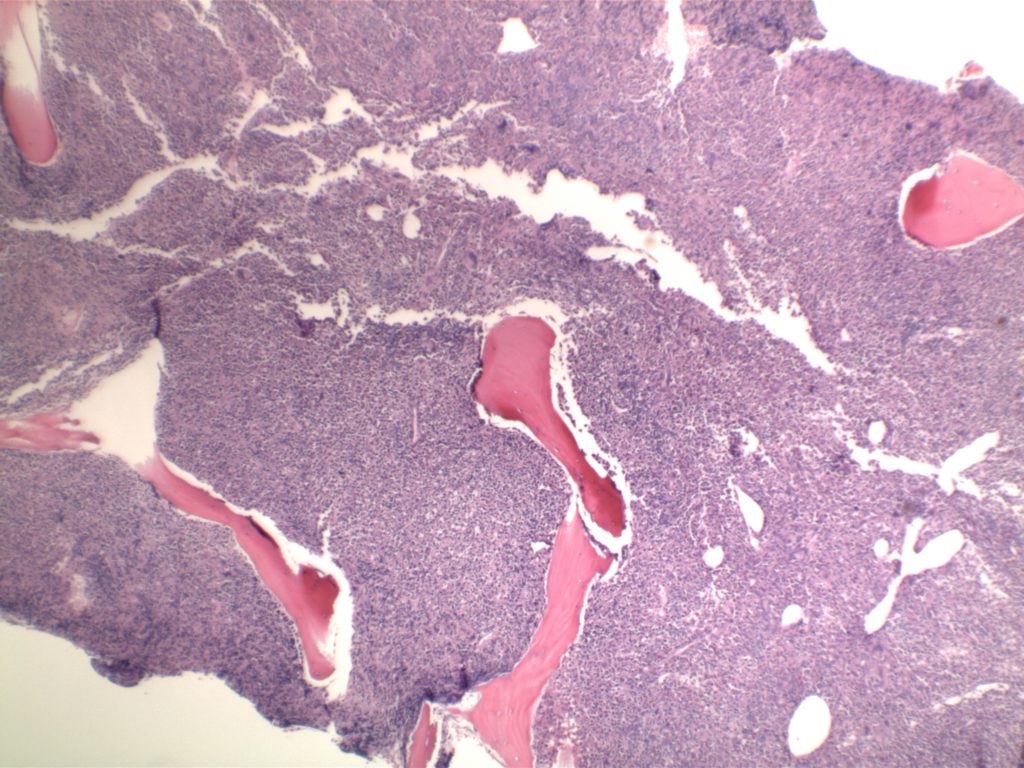
- Hypercellular bone marrow with granulocytic dysplasia (+/- dysplasia in other lineages)
- <20% blasts in PB and BM
- Does not meet diagnostic criteria for BCR-ABL1+ CML, PMF, PV, or ET (if you compare to the criteria for other MPNs, this is a circular argument)
- No PDGFA, PDGFB, FGFR1, or JAK2-PCM1 rearrangement
In the past has been difficult to differentiate from CNL. This category has been somewhat better clarified in the 2016 WHO revision.
- <10% have CSF3R mutation (strong association with CNL, if present should closely examine to exclude CNL – mutation may have therapeutic implications irregardless of diagnosis)
- Not usually associated with JAK2, CALR, or MPL mutations
- Up to 1/3rd of cases have SETBP1 and/or ETNK1 mutations
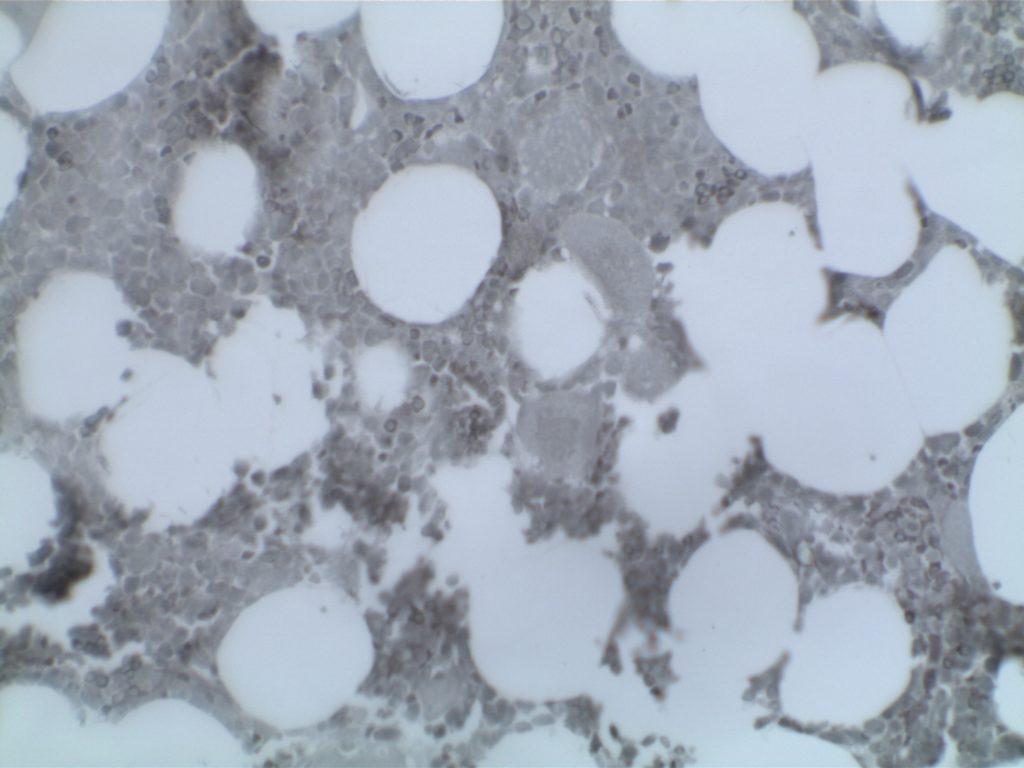
Immunohistochemistry
The use of immunohistochemistry (IHC) in many of the MPN/MDS neoplasms is limited. Identifying an increased blast population is one of the most useful, and may indicate a more aggressive course or transformation to acute myelogenous leukemia (AML). Helpful IHC markers may include:
|
Stain
|
Comment
|
|
CD34 marks immature cells including myeloblasts. In the setting of AML, it is ~70% sensitive. A subset of lymphoblasts may express CD34.
|
|
|
CD117 is a specific myeloid marker, and marks a subset of myeloblasts. The expression is dim, and one often must look at 20-40X to clearly see expression. Mast cells (fried egg looking cell) will have very strong expression.
|
|
|
CD71 marks nucleated erythroid cells. This may be helpful in quantitating and differentiating erythroid cells from myeloid cells. This marker may be set-up as a double stain with CD34.
|
|
|
In the setting of hematopoietic cells, E-Cadherin marks immature erythroid cells. Like CD71, E-Cadherin may be useful to differentiate immature erythroid cells from immature myeloid cells.
|
|
|
TdT is a sensitive lymphoblast (~95%) marker. It is not entirely specific for lymphoblasts, but other markers can help clarify diagnostic difficulties (B and T-cell markers).
|
References
Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127: 2391–2405. doi:10.1182/blood-2016-03-643544
WHO Classification of Tumors of Haematopoietic and Lymphoid Tissues. SH Swerdlow, et al. International Agency for Research on Cancer. Lyon, 2008.
Hematopathology. [edited by] Jaffe, ES. 1st. ed. Elsevier, Inc. © 2011.