
Atypical lobular hyperplasia is a proliferation of epithelial cells in the terminal duct-lobular unit that lacks expression of E-cadherin and fills the lobular unit (but does not expand). Some define ALH as filling or distending <50% of the acini within an affected lobule. There is some variation between experts as the exact differentiating line between ALH and lobular carcinoma in situ (LCIS). It is best to think of ALH and LCIS as representing a morphologic spectrum with filling and distention of lobular acini being the measured characteristic.
In some cases ALH/LCIS may appear similar to DCIS or merge with areas of DCIS. E-cadherin is a helpful marker to differentiate between these lesions. Clinically it is important to differentiate ALH/LCIS from DCIS because LCIS/ALH is an incidental finding on mammogram and represents a risk factor for bilateral breast carcinomas. Management is not through local excision, but surveillance and hormonal therapy dependent upon the type of lesion. DCIS is treated through local excision because these lesions tend to be localized/focal.
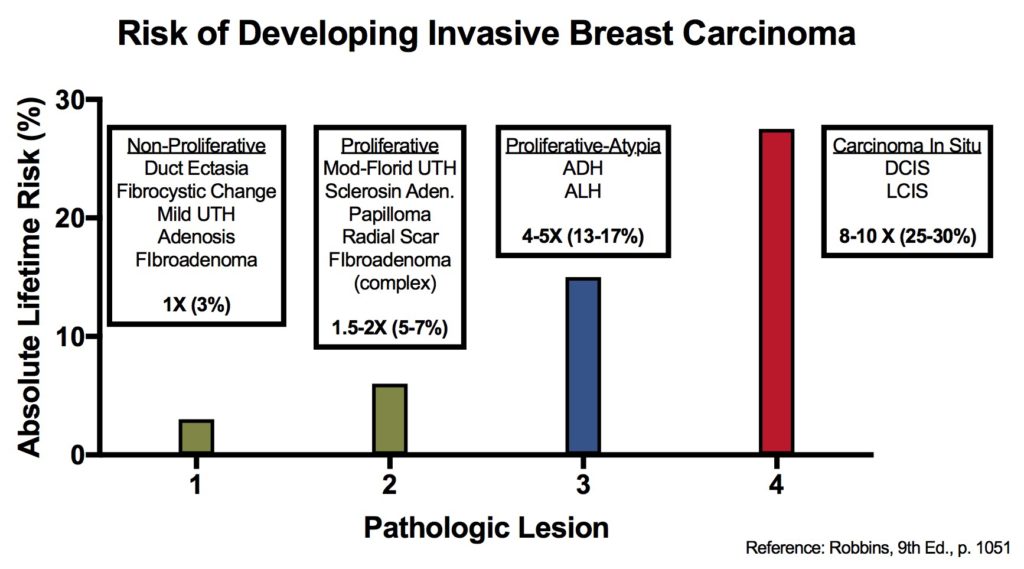
ALH carries an increased risk of developing an invasive breast carcinoma (4-5x relative risk, 13-17% lifetime risk), while LCIS carries an 8-10x increased relative risk, 25-30% lifetime risk). These are the same risks as ALH and DCIS, respectively. Although ALH/LCIS risk is bilateral, while ADH/DCIS tends to be more ipsilateral.
Breast lesions and risk of developing an invasive carcinoma
References
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015. p. 1050-1051