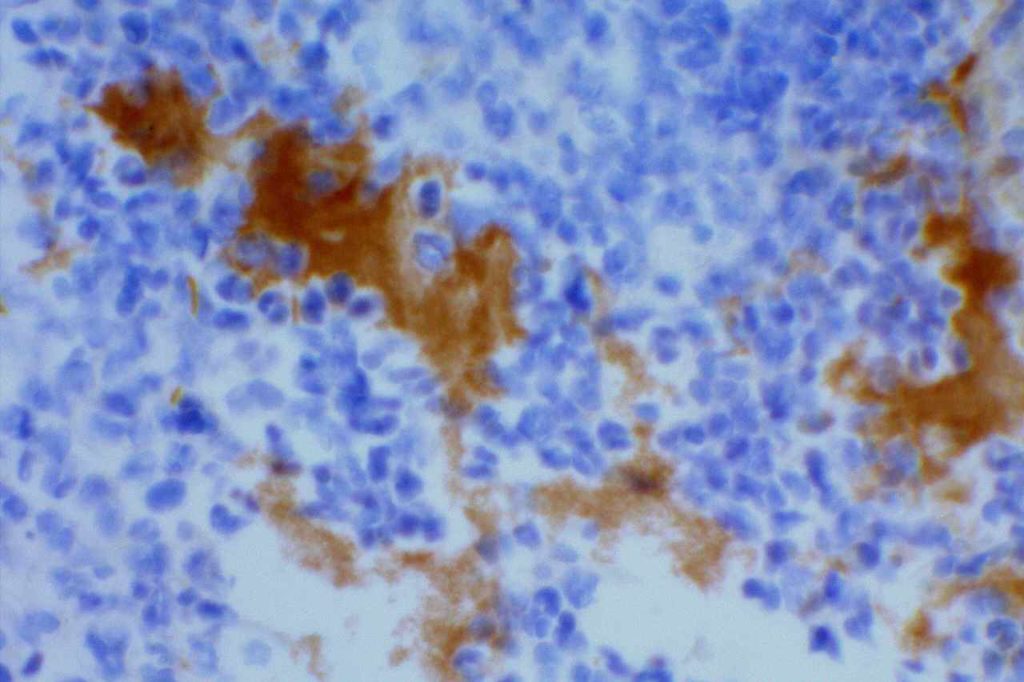
Human herpes virus 8 (HHV-8) is a γ-herpesvirus that infects lymphocytes, bone marrow stromal cells, endothelial cells and keratinocytes, and is implicated as an etiology in multiple neoplastic conditions (usually associated with immunodeficiency). Kaposi’s sarcoma was the first described entity (1994), which was closely associated with HIV infection. While there is still a close association of HHV-8 driven neoplasms with HIV, this is certainly not an exclusive relationship. Interestingly, most of the HHV-8 lymphoproliferative disorders have plasmabalstic differentiation (helpful hint to evaluate for HHV-8 in such cases, especially if associated with immunodeficiency).
Category Archives: G – M Antibodies
Mammaglobin
Mammaglobin is an antibody that marks breast duct-lobular epitheliam, salivary gland epithelium, & skin eccrine epithelium. In neoplastic tissue is may stain cases of breast carcinoma, salivary gland tumors, endocervical CIS, and endometiral carcinoma. GCDFP-15 performs a little better than mammaglobin, and may have a better specificity profile.
MART-1/Melan-A
MART-1/Melan-A has an expression pattern very similar to HMB-45, and these stains are often used interchangeably. It is a sensitive and specific marker for melanocytes and melanocytic derived neoplasms. Like HMB-45, MART-1 is NOT as sensitive compared to S-100 in detecting melanomas with spindled morphology.
LEF1
Lymphoid enhancer-binding factor 1 (LEF1) is a mediator of the Wnt/β-catenin pathway, which regulates cell proliferation and survival, and shows nuclear expression by immunohistochemistry. It is normally expressed in T cells and pre-B cells. Mature B cells do not express LEF1.
MOC-31
MOC-31 is a glycoprotein on the cell-membrane (epithelial glycoprotein 2/epithelial cell adhesion molecule – Ep-CAM) that is widely distributed on epithelial cells and tumor cells. MOC-31 is often used to differentiate adenocarcinoma (93% positive) from mesothelioma (93% negative). Other tumors also typically negative for MOC-31 include: hepatocellular carcinoma (HCC), germ cell tumors, and renal cell (some report up to 50%+) carcinomas. Some tumors may have characteristic staining patterns (e.g. membraneous vs. cytoplasmic or apical).
MUM-1/IRF-4
MUM-1/IRF-4 (multiple myeloma oncogene 1/Interferon Regulatory Factor-4) is a nuclear transcription factor, which is expressed in late stage germinal center cells (as bcl-6 expression begins to be down-regulated) and post-germinal center lymphocytes/plasma cells. Activated T-cells may also express MUM-1.
Lysozyme
Lysozyme (LZ) is similar to myeloperoxidase (MPO) in that they are associated with cytoplasmic bactericidal granules, which are specific for myeloid differentiation. LZ is most useful along with other markers such as MPO and CD117 in identifying case of AML, in which none of the markers are entirely sensitive.
References
Bone Marrow IHC. Torlakovic, EE, et. al. American Society for Clinical Pathology Pathology Press © 2009. pp.161.
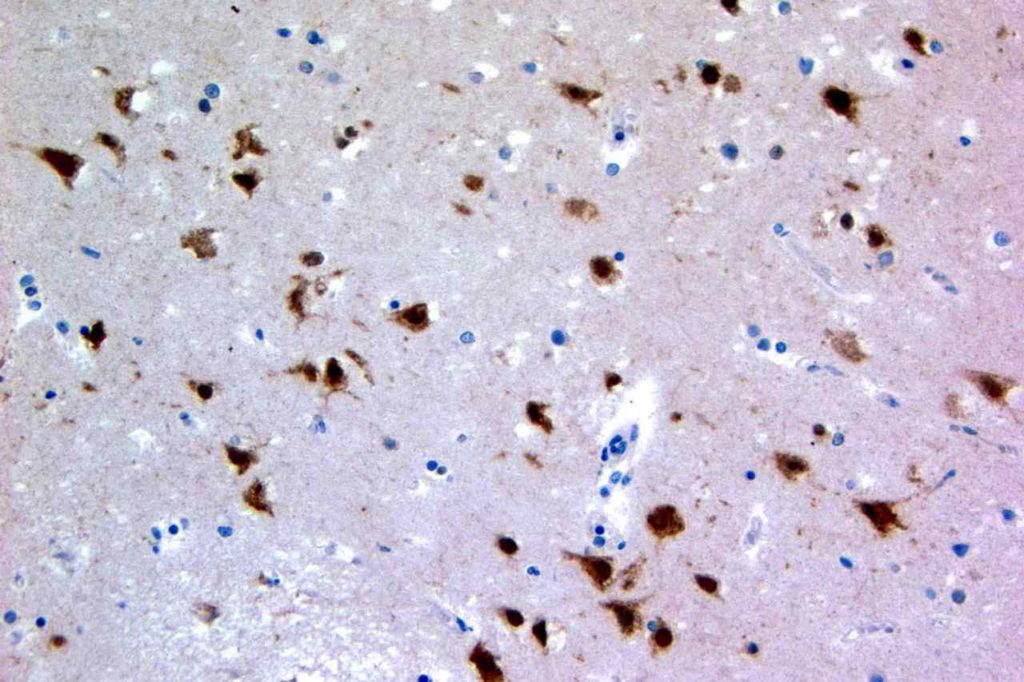
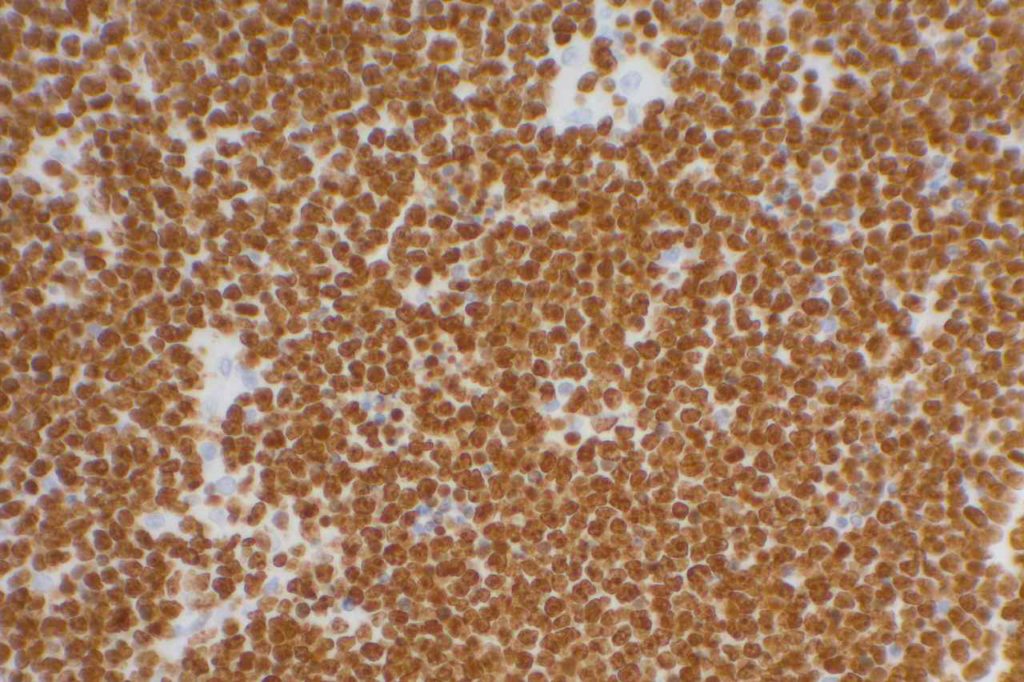
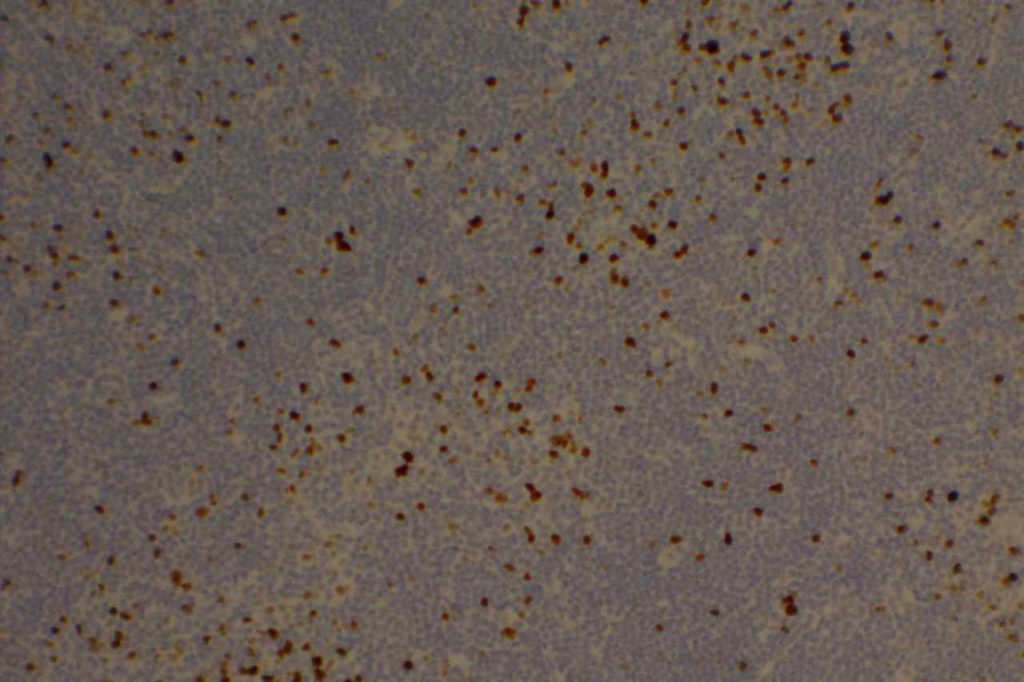
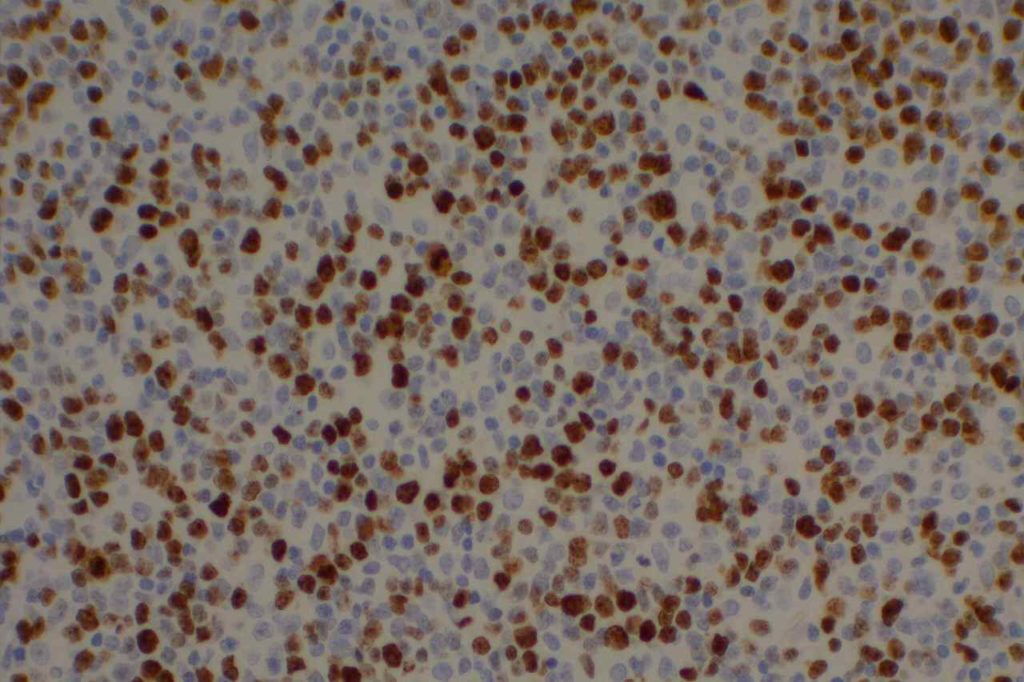
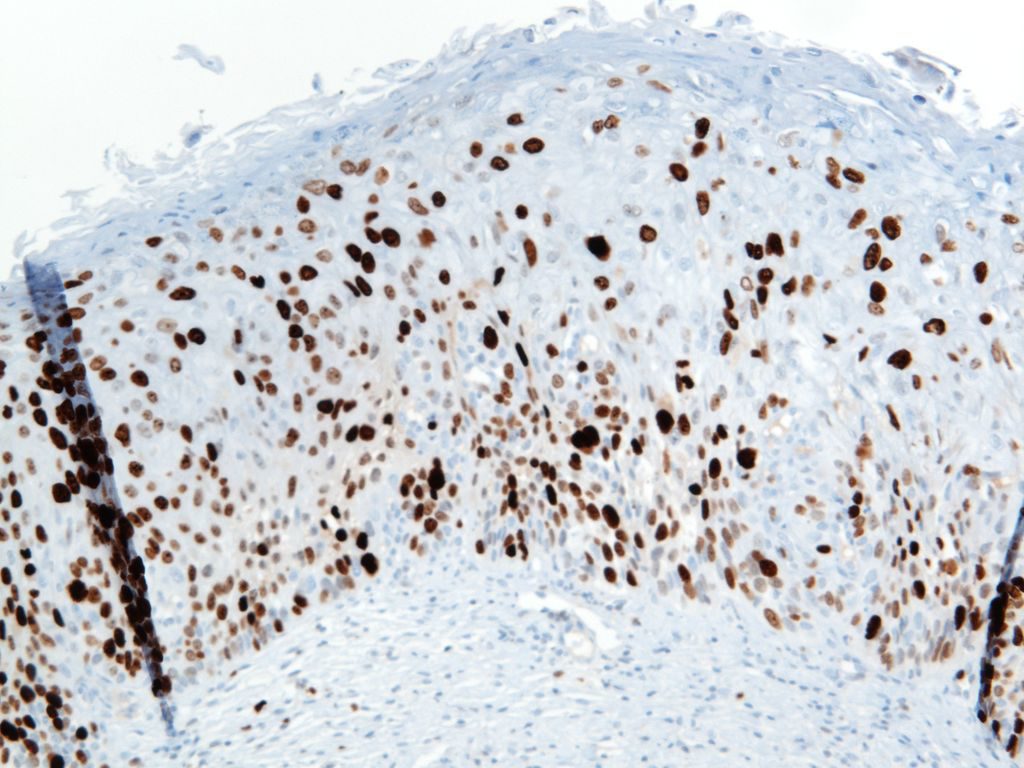
Ki-67
General
Ki-67 is a proliferation marker with nuclear staining. It is expressed in cells in G1, S, G2 and M phases of the cell cycle. This marker is used in many ways, and often carries prognostic information for many malignancies (breast, certain lymphomas, etc.). It is also used as a diagnostic aid in certain difficult cases (e.g. cervical dysplasia, melanocytic tumors, etc.).
When using this stain diagnostically, one should understand the clinical significance for the diagnostic circumstance in which the stain is being used, and have appropriate knowledge of the medical literature with respect to the staining performance in the given clinical-pathologic setting. For example low grade lymphomas would be expected to have a relatively low-proliferation staining index (<30%), whereas Burkitt Lymphoma would have a high staining index (>95%).
Clone: MIB-1 (most common)
Photomicrographs
Reference:
Katzenberger, T., Petzoldt, C., Höller, S., Mäder, U., Kalla, J., Adam, P., et al. (2006). The Ki67 proliferation index is a quantitative indicator of clinical risk in mantle cell lymphoma. Blood, 107(8), 3407. doi:10.1182/blood-2005-10-4079
McCall, C. M., Shi, C., Cornish, T. C., Klimstra, D. S., Tang, L. H., Basturk, O., et al. (2013). Grading of well-differentiated pancreatic neuroendocrine tumors is improved by the inclusion of both Ki67 proliferative index and mitotic rate. The American Journal of Surgical Pathology, 37(11), 1671–1677. doi:10.1097/PAS.0000000000000089
Bone Marrow IHC. Torlakovic, EE, et. al. American Society for Clinical Pathology Pathology Press © 2009. pp. 209.
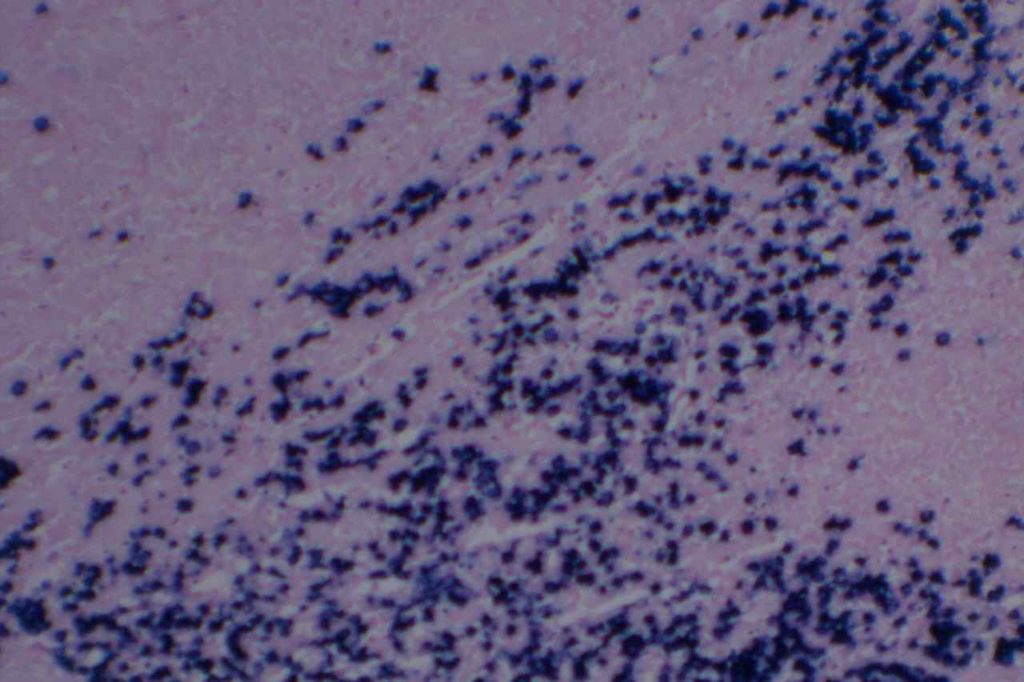
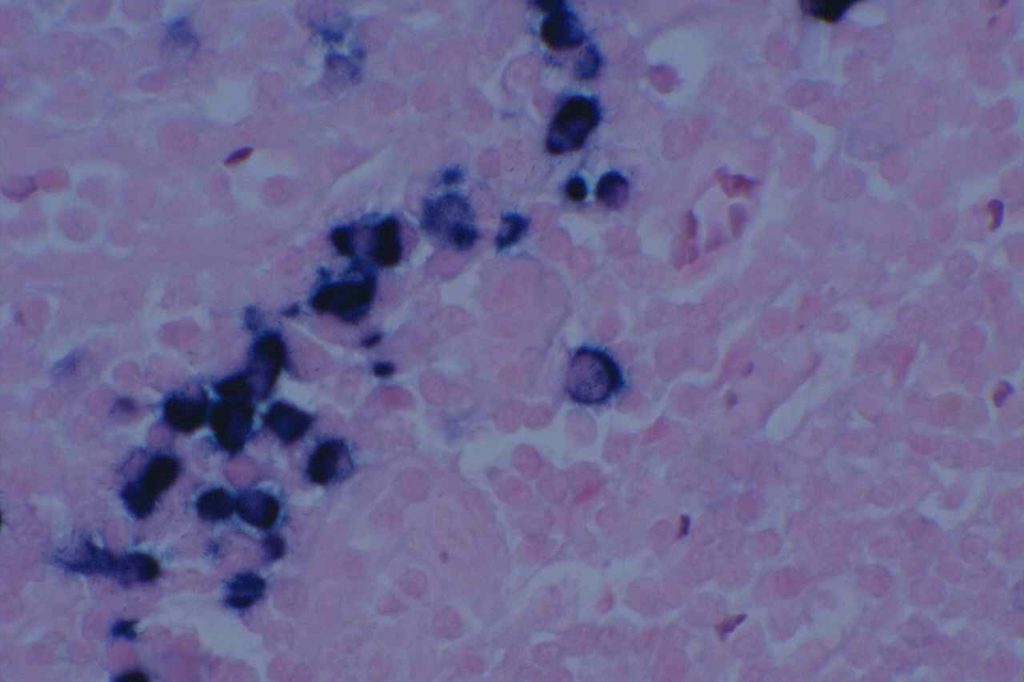
Kappa/Lambda
Kappa/Lambda (K/L) may be performed by immunohistochemistry (IHC) or in situ hybridization (ISH). K/L studies is primary used in the evaluation of plasma cell disorders or lymphoproliferative disorders containing some level of plasmacytoid differentiation. In tissue sections IHC for K/L often produces a large amount of background staining, which makes its use more difficult on a day-to-day basis compared to ISH (much less background).
The second big issue in K/L staining is that it is often performed on decalcified bone marrow biopsy core sections. The decalcification process may cause significant issues in the sensitivity of both IHC and ISH. As an alternative, always making a clot section on bone marrow specimens may greatly increase diagnostic yield and reliability.
Determination of monoclonality of plasma cells can sometimes be challenging. Historically, most consider a K:L ratio <0.5 or >4.0 to be indicative of monoclonality. Like almost everything in pathology, holding to a specific and tight threshold may put one in a perilous position in making a diagnosis. By flow cytometry, Samoszuk, et. al found that K:L ratios <0.7 and >5.5 were optimum for discriminating between lymphoma and benign hyperplasia (false negative rate= 27%, and false positive rate= 6%).
Evaluating K:L ratios in tissue sections is generally analogous to flow cytometry. Normally, there are 2-4 Kappa plasma cells to every Lamdda plasma cell. A ratio of K:L > 8:1 or a L:K ratio > 4:1 is strongly suggestive of a monoclonal plasma cell population.
Practically, if K:L ratio is no “obviously” monoclonal on ISH/IHC, it may be best to identify it as a kappa or lambda predominate population and correlate with other laboratory, radiologic and clinical findings. A significant pitfall may occur when either the kappa or lambda stain doesn’t work, and the case looks like a monoclonal population. Even in “obvious” monoclonal cases, one should be able to find a rare kappa or lambda staining plasma cell. If not, then the maker should be repeated.
Photomicrographs
References
Parker, A., et. al. “Best Practice in Lymphoma Diagnosis and Reporting.” British Committee for Standards in Haematology, Royal College of Pathologists. April, 2010.
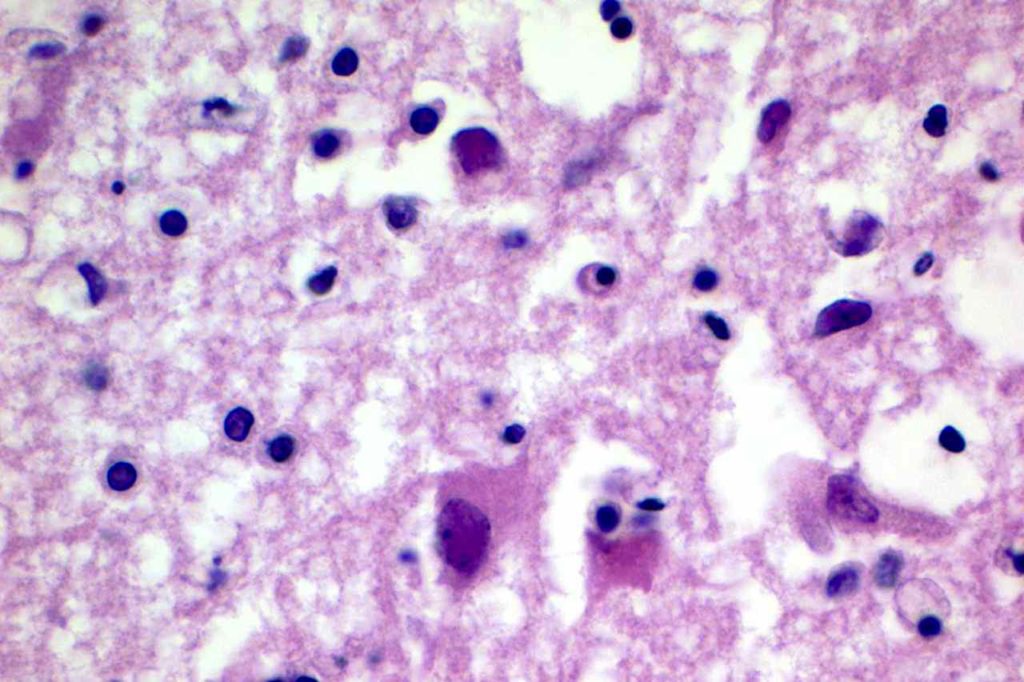
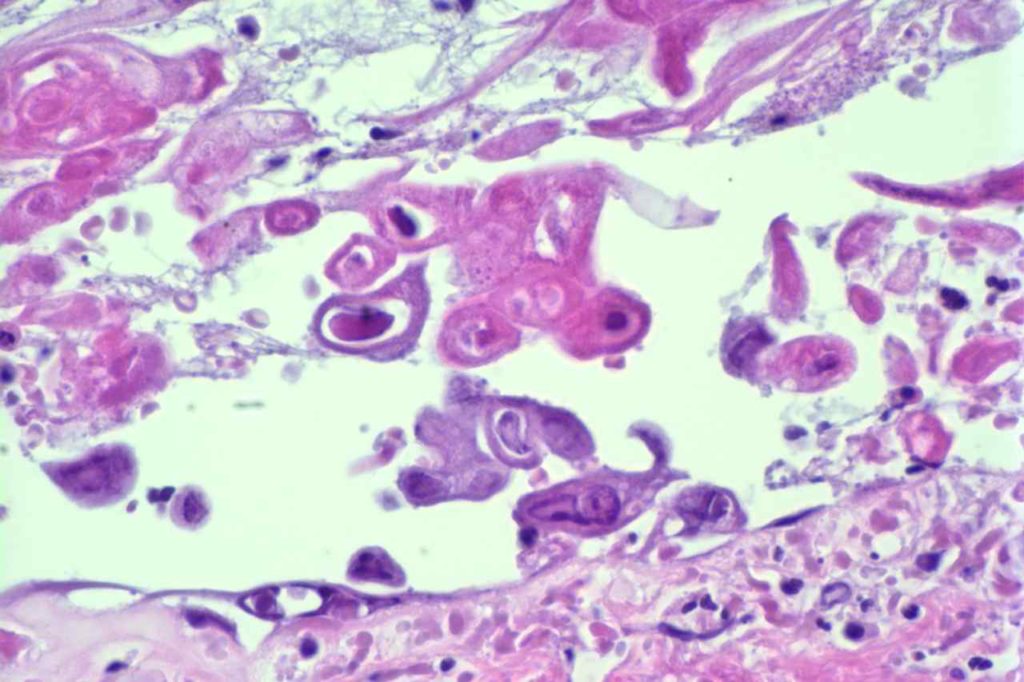
Herpes Simplex Virus (HSV)
Herpes Simplex Virus (HSV) is a virus, which causes a painful skin/mucosal blistering disorder that can involve numbers areas including genitalia, lips, esophagus, and skin. Immunohistochemistry (IHC) antibodies for HSV-1 and HSV-2 are available for testing in paraffin embedded tissue. In general, HSV-1 infections are more common above the diaphragm, and HSV-2 are more common below the diagram. While the availability of HSV-1 specific and HSV-2 specific antibodies for testing might suggest they are highly specific. In the author’s experience, there is a lot of cross reactivity between the HSV-1 and HSV-2 antibodies, and one should not consider positivity as definitively specific.
Photomicrographs