Monoclonal and polyclonal antibodies are available to H. pylori for use in paraffin embedded tissue. While less specific, other stains (e.g. silver stains, Giemsa, modified Steiner, etc.) may be used to highlight the bacterial organisms. IHC stains provide the most sensitive and specific marker for identification. Additionally, IHC stains for H. pylori have much lower background than special stains, making it easier for the pathologist to make the diagnosis.
Stain Interpretation
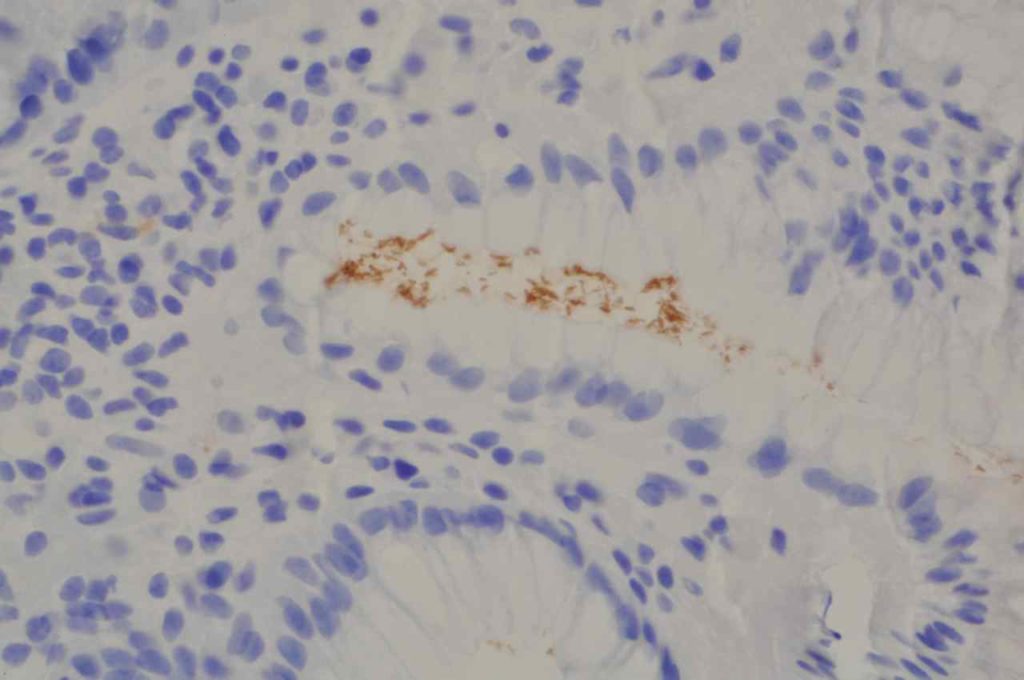
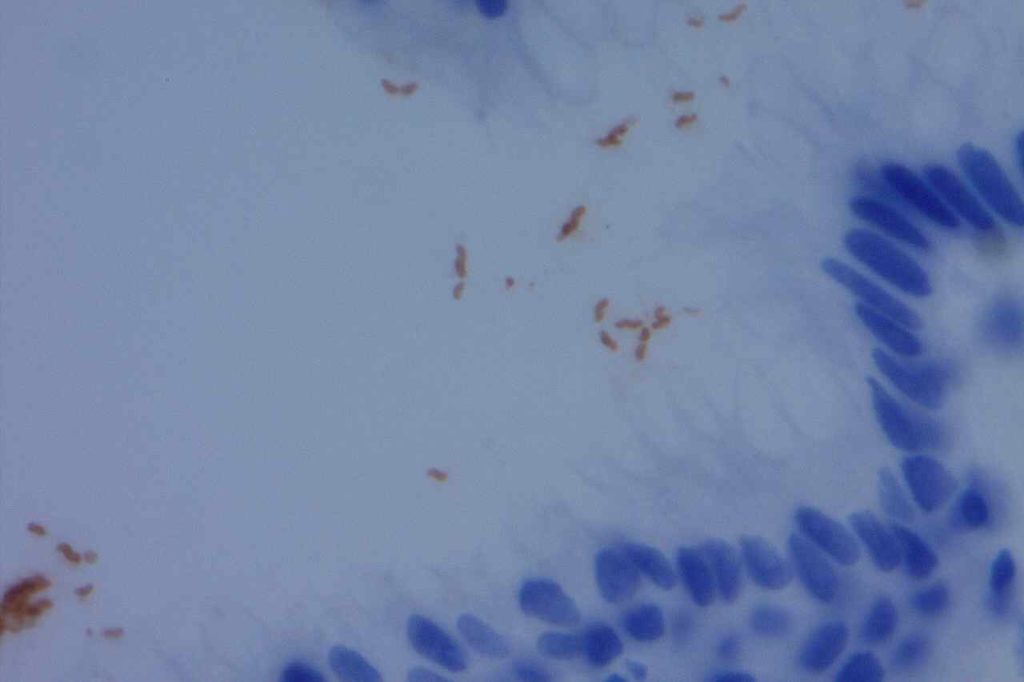
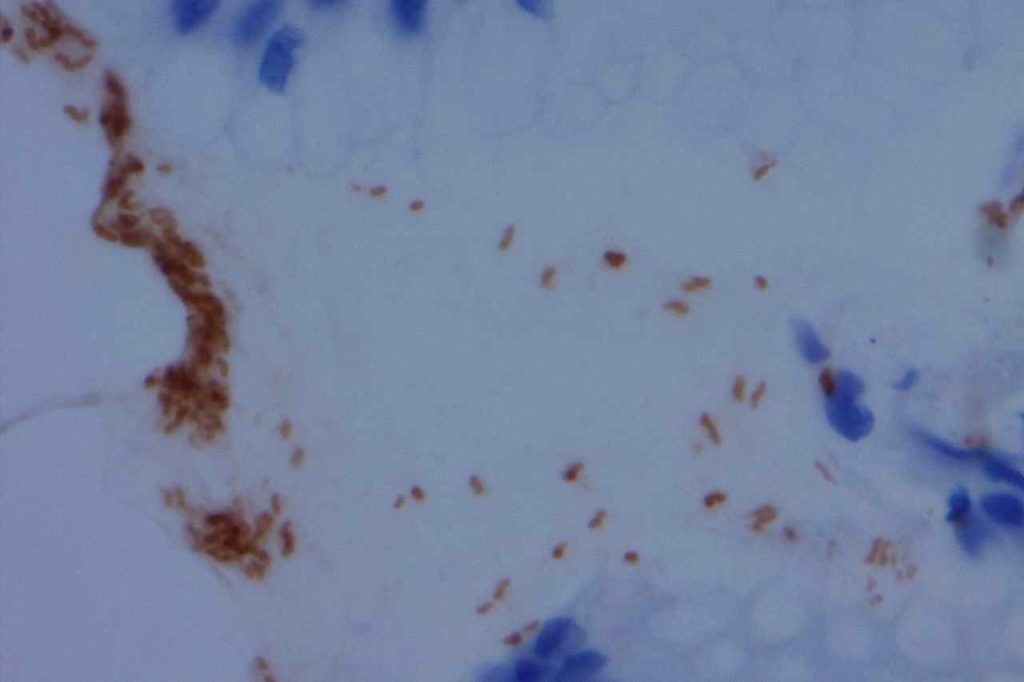
For a case to be positive, there must be staining and bacterial morphology (curvilinear organisms). There are several pitfalls to be aware of to interpret H. pylori stains:
“Junk Staining” on the surface as a result of neutral red or other pigmented stains used as the time of grossing to help visualize tissue while cutting. This most commonly occurs when stains used at the grossing station are not filtered regularly (or are just old) with subsequent precipitate material.
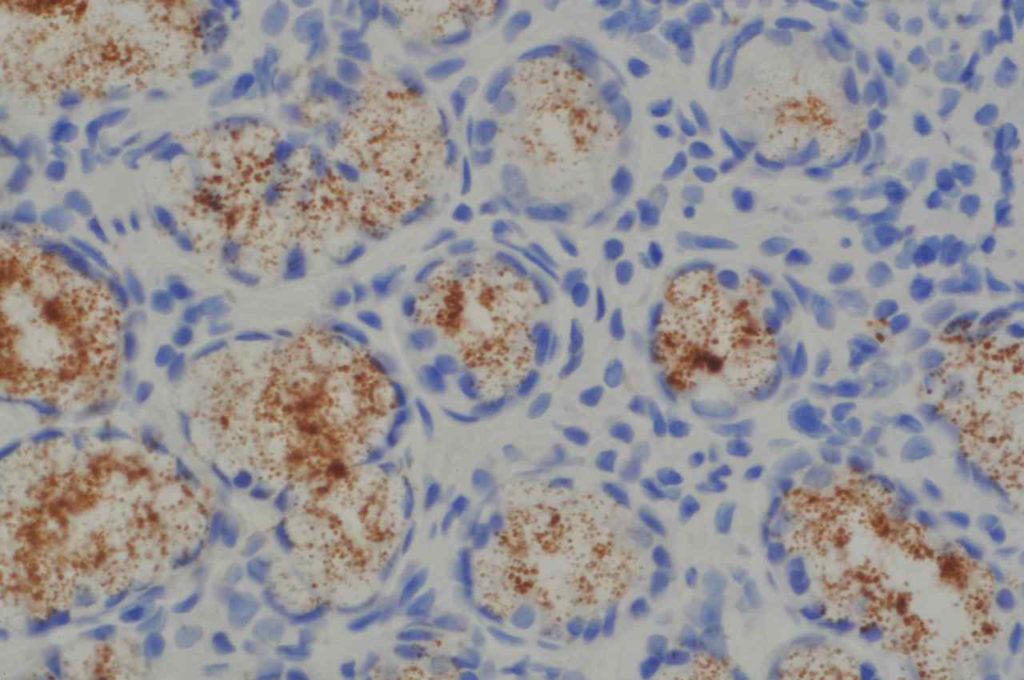
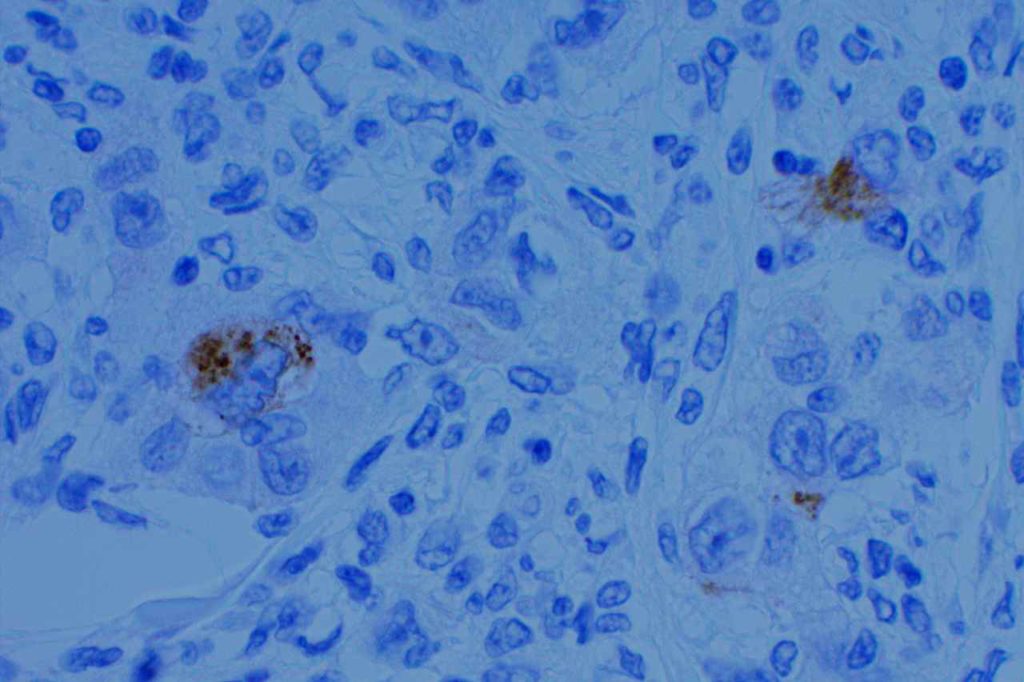
Some antibodies (e.g. Novocastra monoclonal) may show cross-reactivity with cytoplasmic antral gland granules. This is most confusing when the granules are dislodged from the cytoplasmic location during the biopsy procedure and are distributed along the mucosal surface. They have a characteristic appearance of variably sized round granules.
Stain Sensitivity and Specificity (Hartman, et al)
Stain
Sensitivity
Specificity
H&E
83%
100%
Giemsa
62%
97%
Warthin-Starry
62%
98%
IHC Staining
97-100%
100%
General Comment
The Rodger C. Haggitt Gastrointestinal Pathology Society has published a consensus recommendation that special stains to evaluate for Helicobacter organisms are appropriate when there is chronic gastritis or chronic active gastritis without evidence of organisms on routine H&E sections. Routine performance of special stains upfront on all biopsies for Helicobacter is NOT recommended. (Batts, et al)
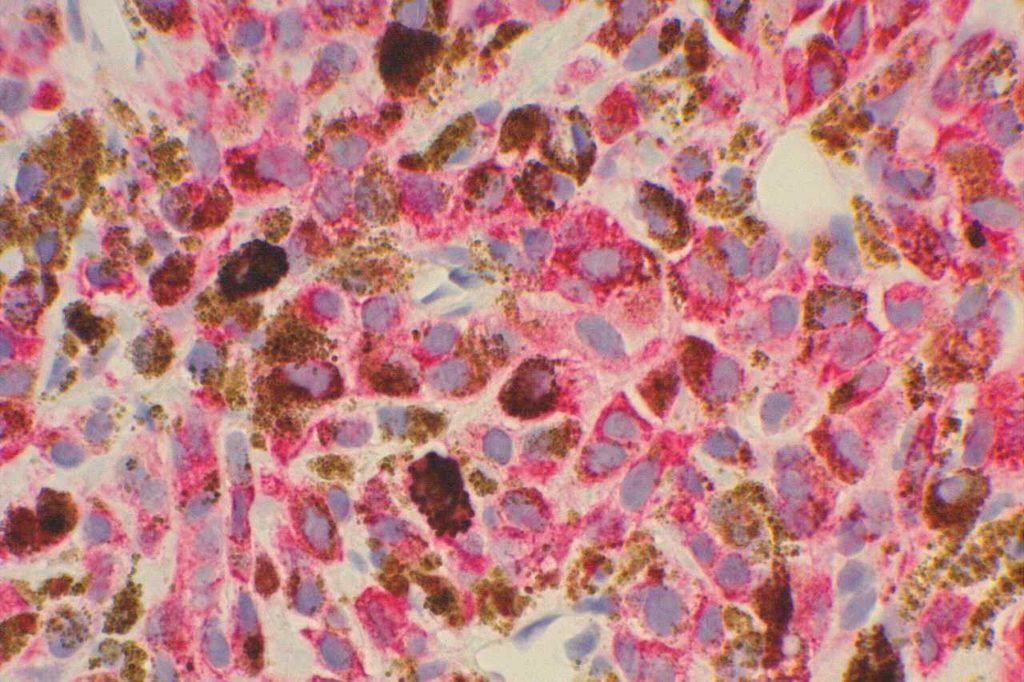
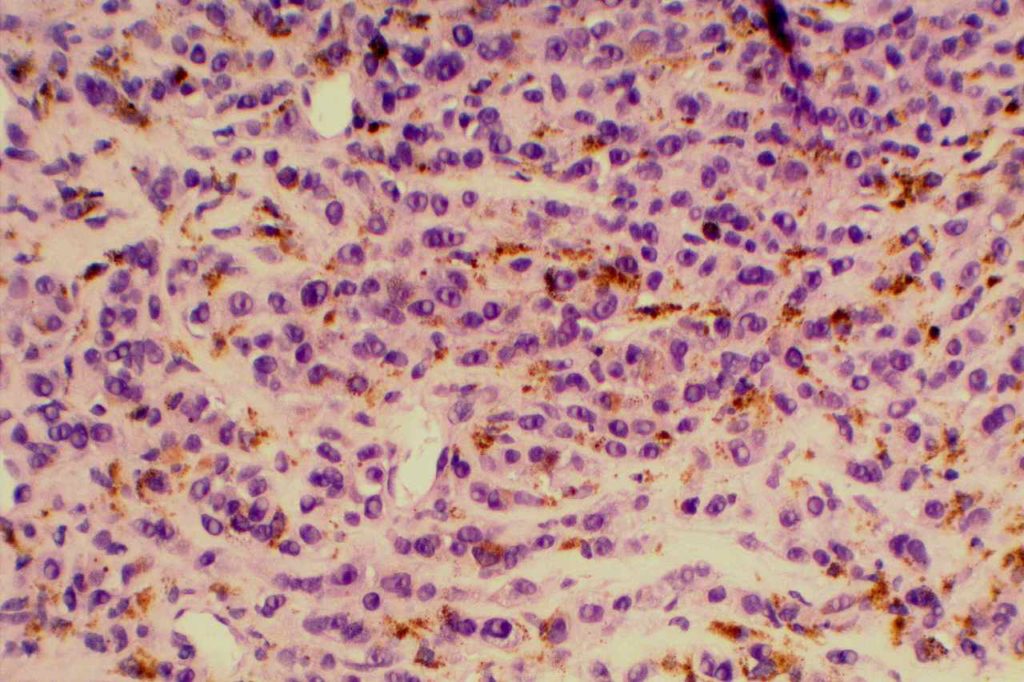
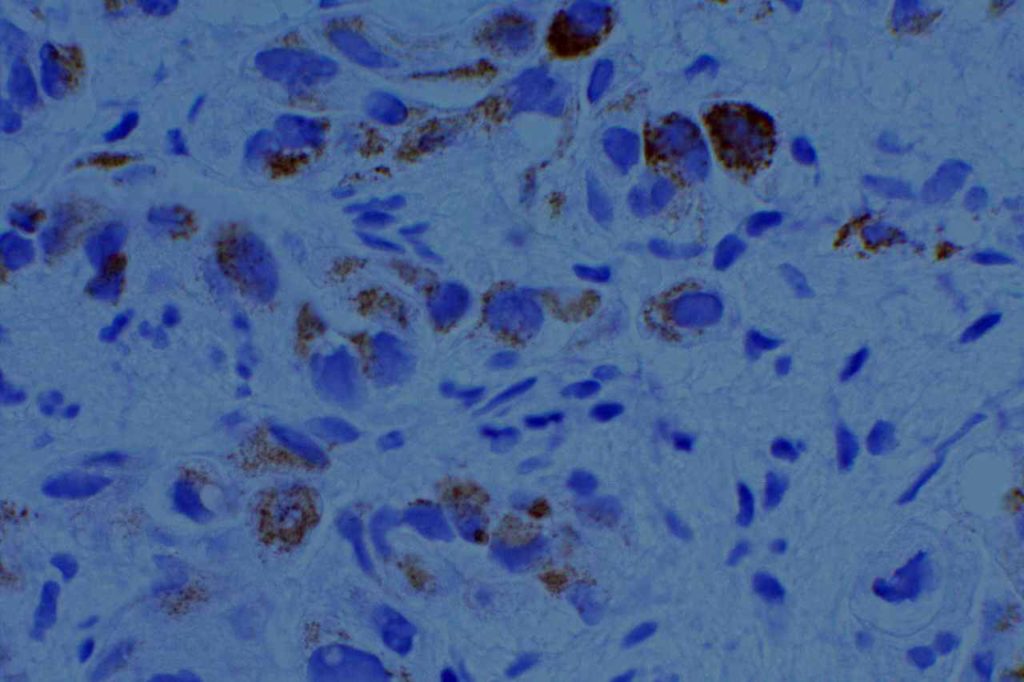
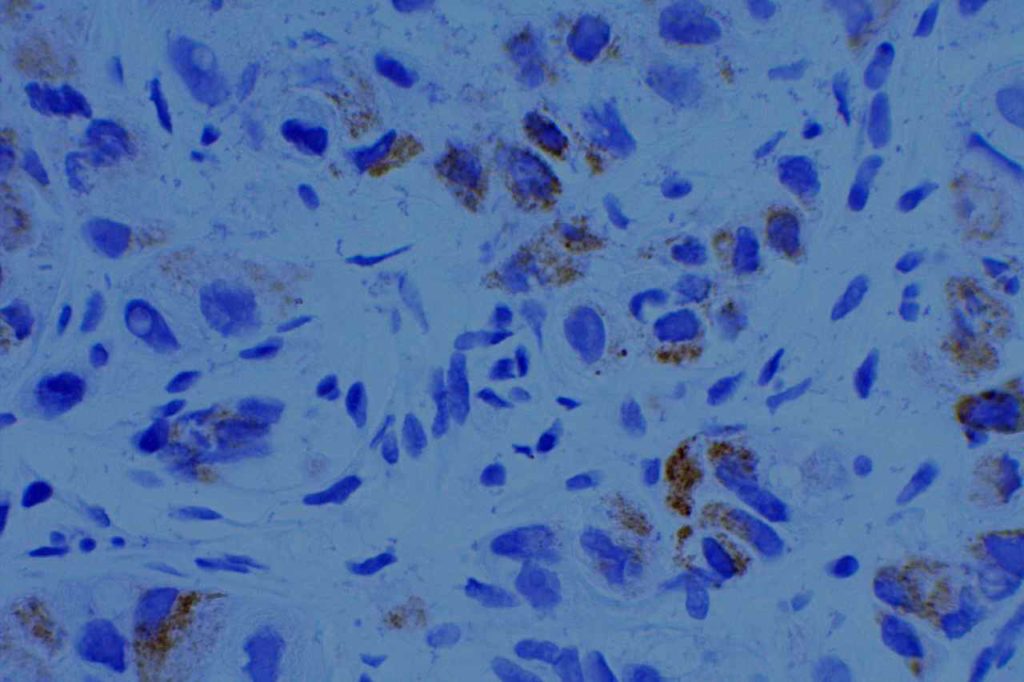
Please see the image example for demonstration of proper staining and artifacts.
H. pylori IHC stain highlighting Helicobacter organisms.H. pylori IHC stain highlighting Helicobacter organisms.H. pylori IHC stain highlighting Helicobacter organisms.H. pylori (monoclonal) IHC stain highlighting granules in antral glands. This should not be misinterpreted as positive for H. pylori organisms. Round granules from these glands can be displaced during biopsy procedure, which can be located on the mucosal surface causing further confusion.
References:
Hartman, D. J., & Owens, S. R. (2012). Are routine ancillary stains required to diagnose helicobacter infection in gastric biopsy specimens?: an institutional quality assurance review. American Journal of Clinical Pathology, 137(2), 255–260. doi:10.1309/AJCPD8FFBJ5LSLTE
Riba, A. K., Ingeneri, T. J., & Strand, C. L. (2011). Improved Histologic Identification of Helicobacter pylori by Immunohistochemistry Using a New Novocastra Monoclonal Antibody. Laboratory Medicine, 42(1), 35–39. doi:10.1309/LMAGPAENJKNARI4Z
Batts, K. P., Ketover, S., Kakar, S., Krasinskas, A. M., Mitchell, K. A., Wilcox, R., et al. (2013). Appropriate use of special stains for identifying Helicobacter pylori: Recommendations from the Rodger C. Haggitt Gastrointestinal Pathology Society. The American Journal of Surgical Pathology, 37(11), e12–22. doi:10.1097/PAS.0000000000000097
HMB-45 (Human Melanoma Black) is a monoclonal antibody to melanosomal glycoprotein gp100, and is relatively specific for melanocytes. The staining pattern is cytoplasmic. Similar to MART1, HMB-45 is less sensitive for melanoma when it has a spindle cell pattern. S-100 (less specific) is a better screening marker than HMB-45 or MART1. HMB-45 is better as a confirmatory marker.
HMB45 will stain: angiomyolipoma, melanoma, soft part sarcoma, sugar tumor of lung, lymphangiomyomatosis, pheochromocytoma (30%), pigmented nerve sheath tumors, and benign nevi / melanocytes. It is also important to understand that some histiocytes in lymph nodes may stain with HMB-45, which must be differentiated from metastatic melanoma cells. At least some histiocytes stained with HMB-45 in 50% of lymph nodes in a study by Hutchens, KA, et al.
HMB-45 will mark melanocytes and melanocytic derived neoplasms, but is not diagnostic in and of itself of anything abnormal. Dysplasia/neoplasia can only be diagnosed on the H&E slide after confirming morphology and/or melanocytic cell distribution with IHC analysis.
Photomicrograph
HMB-45 expression in melanoma. Red chromogen if helpful in distinguishing tumor cells from non-tumor pigmented cells.HMB-45 expression in melanoma.
Reference
Hutchens, K. A., Heyna, R., Mudaliar, K., & Wojcik, E. (2013). The new AJCC guidelines in practice: utility of the MITF immunohistochemical stain in the evaluation of single-cell metastasis in melanoma sentinel lymph nodes. The American Journal of Surgical Pathology, 37(6), 933–937. doi:10.1097/PAS.0b013e3182815574
Kucher, C., Zhang, P. J., Acs, G., Roberts, S., & Xu, X. (2006). Can Melan-A replace S-100 and HMB-45 in the evaluation of sentinel lymph nodes from patients with malignant melanoma? Applied Immunohistochemistry & Molecular Morphology : AIMM / Official Publication of the Society for Applied Immunohistochemistry, 14(3), 324–327.
HER2 (Human Epidermal growth Factor Receptor 2), which is also known as c-erb2, net, ERBB2, and CD340 is a member of the human epidermal growth factor receptor family (HER1, HER2, HER3, and HER4). Interestingly HER1 is also known as EGFR (epidermal growth factor receptor).
HepPar-1 is a mitochondrial antigen present in normal hepatocytes, and is a relatively specific marker for hepatic origin. It also stains approximately 80-100% of hepatocellular carcinomas. It is most commonly used to help identify tumors of primary hepatic origin, and exclude cholangiocarcinoma in the differential diagnosis.
Interpretation
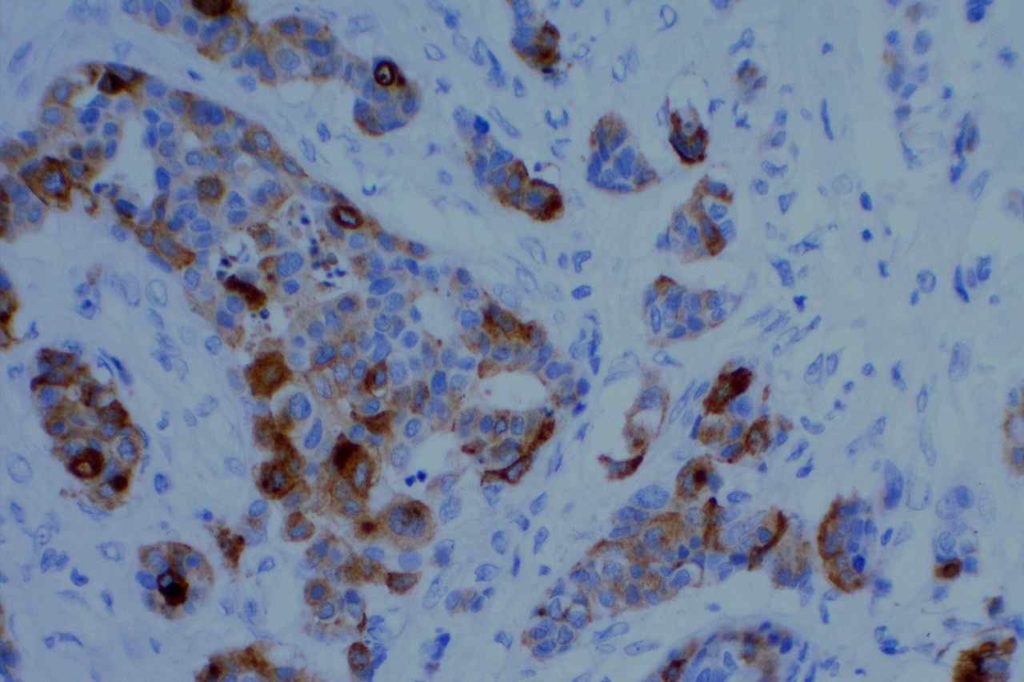
The staining pattern is granular and cytoplasmic in location. The staining pattern can be heterogeneous ranging from focal (<5%) in poorly differentiated HCC to strong diffuse staining in well-differentiated HCC. As with most issues in pathology and IHC, less differentiated lesions more often need IHC, which tend to perform less-optimally than described in the literature (case selection bias). Also beware of focal staining of benign entrapped hepatocytes.
Specificity
HepPar-1 is not a pertfectly specific marker for HCC. One study (Wee) notes specificity as 73% with non-hepatic tumors including adenocarcinomas from lung, gallbladder, pancreas, stomach, small intestine, adenoma of colon, adrenal gland carcinoma, paraganglioma, and melanoma showing expression. Other studies show the specificity near 90% for HCC.
Up to 25% (probably <10% overall) of lung carcinomas (mostly adenocarcinomas) have been noted to have HepPar1 expression (cytoplasmic and granular). The expression pattern may be focal/patchy, but these tumors also typically express TTF-1.
Use of HepPar-1 as part of a panel (and clinical-radiologic correlation) is recommended for optimal interpretation.
Wee, A. (2006). Diagnostic utility of immunohistochemistry in hepatocellular carcinoma, its variants and their mimics. Applied Immunohistochemistry & Molecular Morphology : AIMM / Official Publication of the Society for Applied Immunohistochemistry, 14(3), 266–272.
Allende, D., & Yerian, L. (2009). Immunohistochemical Markers in the Diagnosis of Hepatocellular Carcinoma. Pathology Case Reviews, 14(1), 40–46.
Yousem, S. A., Lale, S., & Dacic, S. (2013). HepPar-1 expression in primary lung adenocarcinoma. American Journal of Clinical Pathology, 140(2), 225–230. doi:10.1309/AJCP4MXTNQRVOE2T
Minervi el al., 1997.
Chu et al., Am J Surg Pathol 26:978-88, 2002.
L. Lamps. “The Differential Diagnosis of Hepatic Tumors.” UAMS, Lecture, 2005.
Gross Cystic Disease Fluid Protein 15 (GCDFP-15) is a marker derived from breast epithelium secretions. It is a marker of apocrine differentiation. In the setting diagnostic pathology, GCDFP-15 is very specific for breast carcinoma. Most basal-like breast carcinomas do not express GCDFP-15 or Mammaglobin. It also marks salivary and sweat gland tumors, but this rarely is in the differential diagnosis with breast carcinoma.
The sensitivity for breast carcinomas is in the range of 50-70%.
Common expression patterns in carcinoma [Dennis, et al and Striebel et al]:
Tumor
(%)
Breast
50-70%
Colon
<5%
Lung
up to 5%
Ovary
<5%
Pancreas
<5%
Stomach
<5%
Prostate
~10%
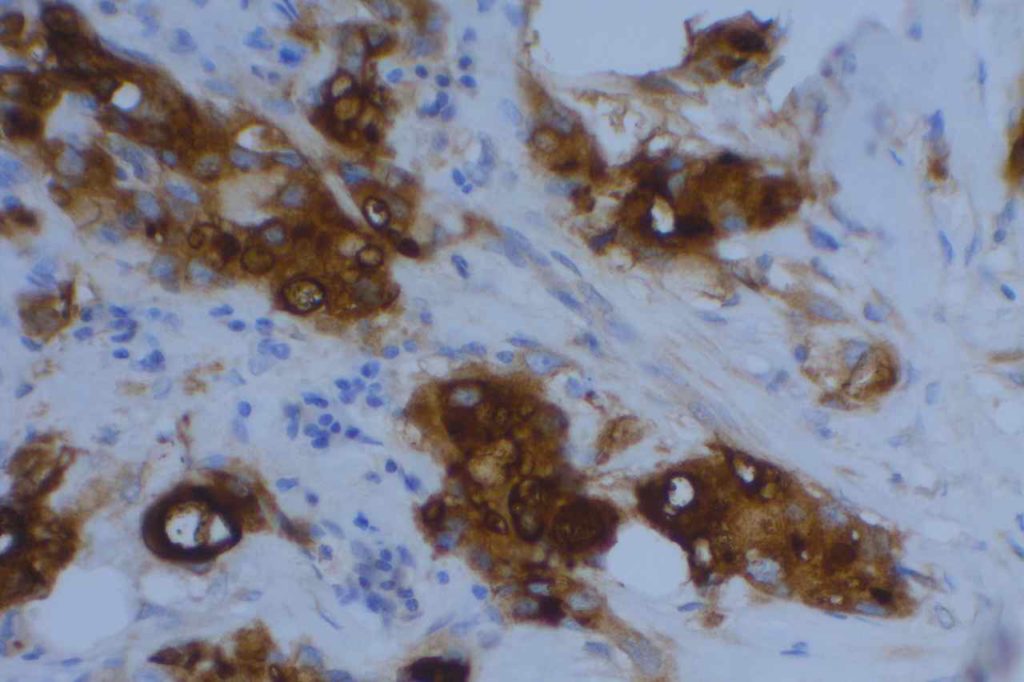
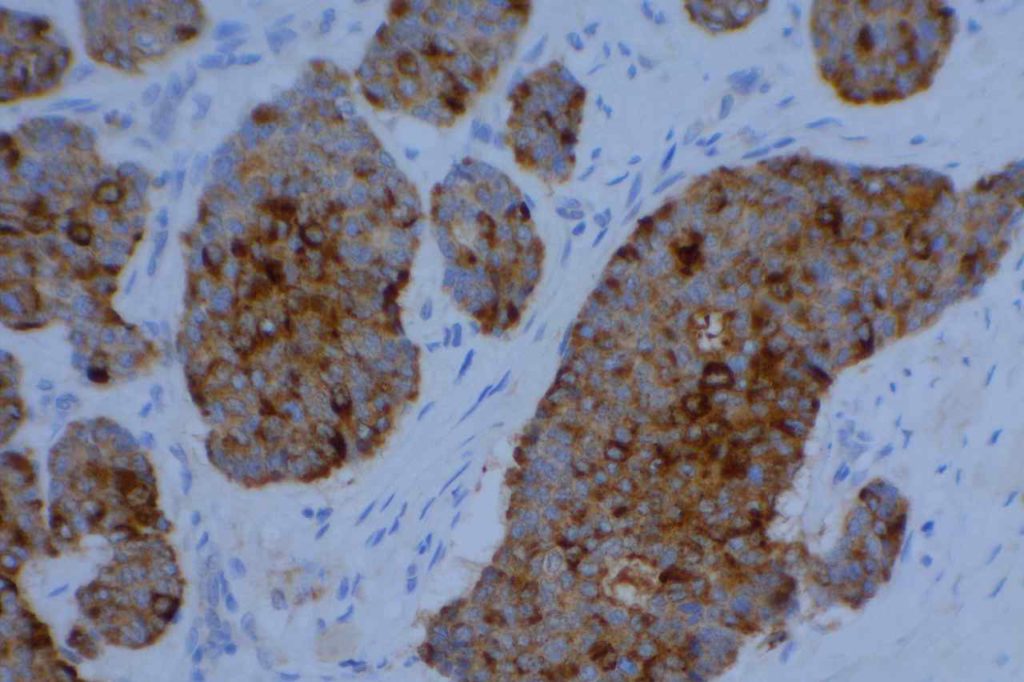
Photomicrographs
GCDFP-15 – Breast CarcinomaGCDFP-15 – Breast CarcinomaGCDFP-15 – Breast CarcinomaGCDFP-15 – Breast Carcinoma
References
Dennis, J. L., Hvidsten, T. R., Wit, E. C., Komorowski, J., Bell, A. K., Downie, I., et al. (2005). Markers of adenocarcinoma characteristic of the site of origin: development of a diagnostic algorithm. Clinical Cancer Research : an Official Journal of the American Association for Cancer Research, 11(10), 3766–3772. doi:10.1158/1078-0432.CCR-04-2236
Striebel, J. M., & Yousem, S. A. (2008). Gross Cystic Disease Fluid Protein – (GCDFP-15): Expression in Primary Lung Adenocarcinoma. The American Journal of Surgical Pathology, 00(00), 7.
Lewis, G. H., Subhawong, A. P., Nassar, H., Vang, R., Illei, P. B., Park, B. H., & Argani, P. (2011). Relationship between molecular subtype of invasive breast carcinoma and expression of gross cystic disease fluid protein 15 and mammaglobin. American Journal of Clinical Pathology, 135(4), 587–591. doi:10.1309/AJCPMFR6OA8ICHNH
Granzyme B is a cytoplasmic marker for cytotoxic T lymphocytes. It is used as a marker along with TIA-1 to prove cytotoxic differentiation. It is expressed in normal cytotoxic T cells and certain T cell neoplasms derived from cytotoxic T cells.
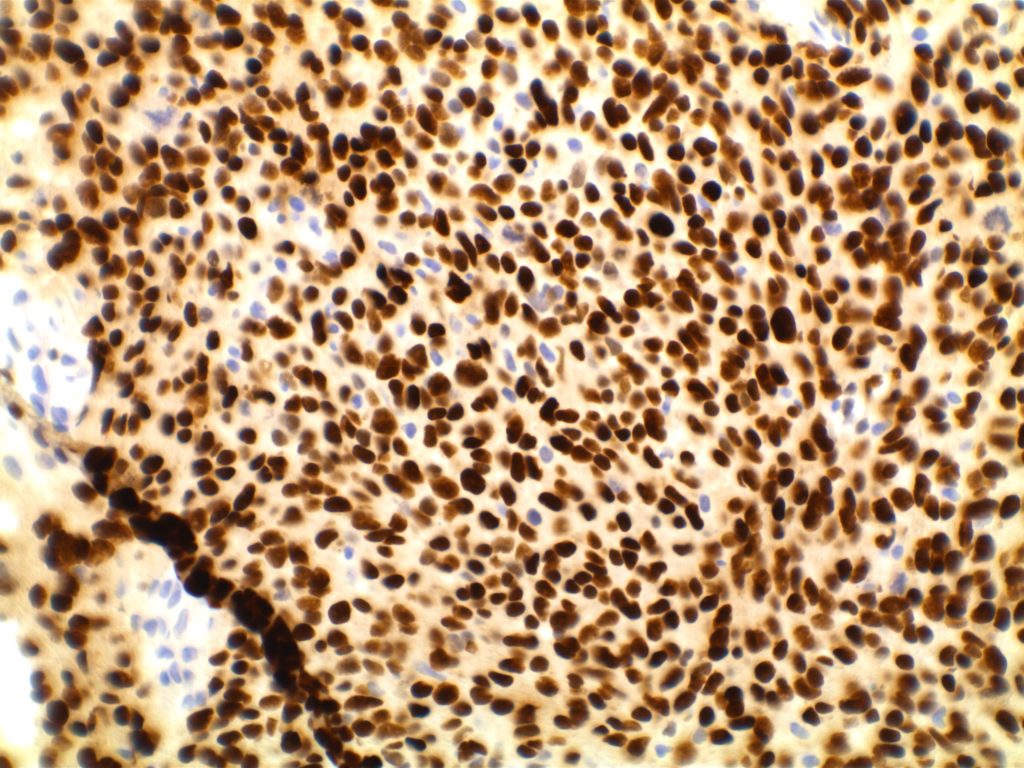
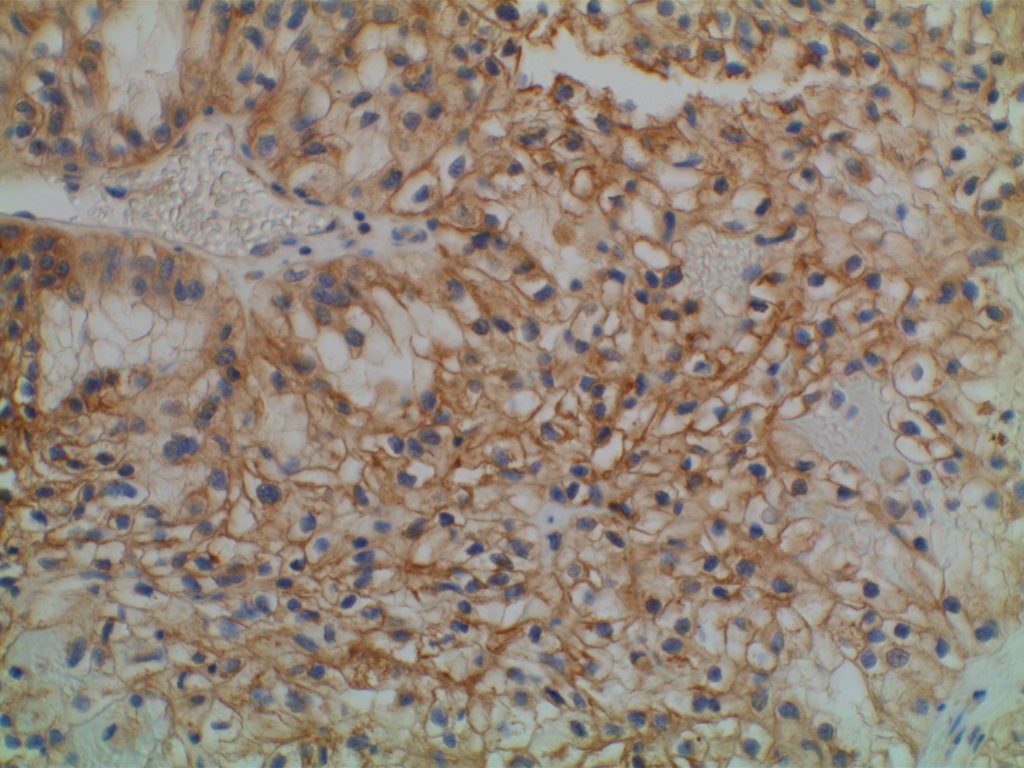
GATA-3 is a member of a subfamily of zinc finger transcription proteins, which has been found to be highly expressed in breast (>90%) (especially lunimal A breast carcinomas) and urothelial carcinomas (>80%). Current evidence suggests that this marker has a better balance of sensitivity and specificity for breast carcinoma than GCDFP-15 and mamaglobin (MGB). Especially, in the setting of ER-negative tumors. GATA-3 use should be considered as part of IHC panels in the setting of carcinoma of unknown primary site. (Lin, et al) Mccluskey, et al. found high GATA-3 expression to be associated with favorable survival and relapse free course in advanced cases.
GATA-3 may also have a role in the evaluation of possible primary bladder tumors. As with most IHC markers, there are very few “silver bullets,” and interpretation should take into consideration the clinical-radiologic context along with the known performance characteristics of the antibody.
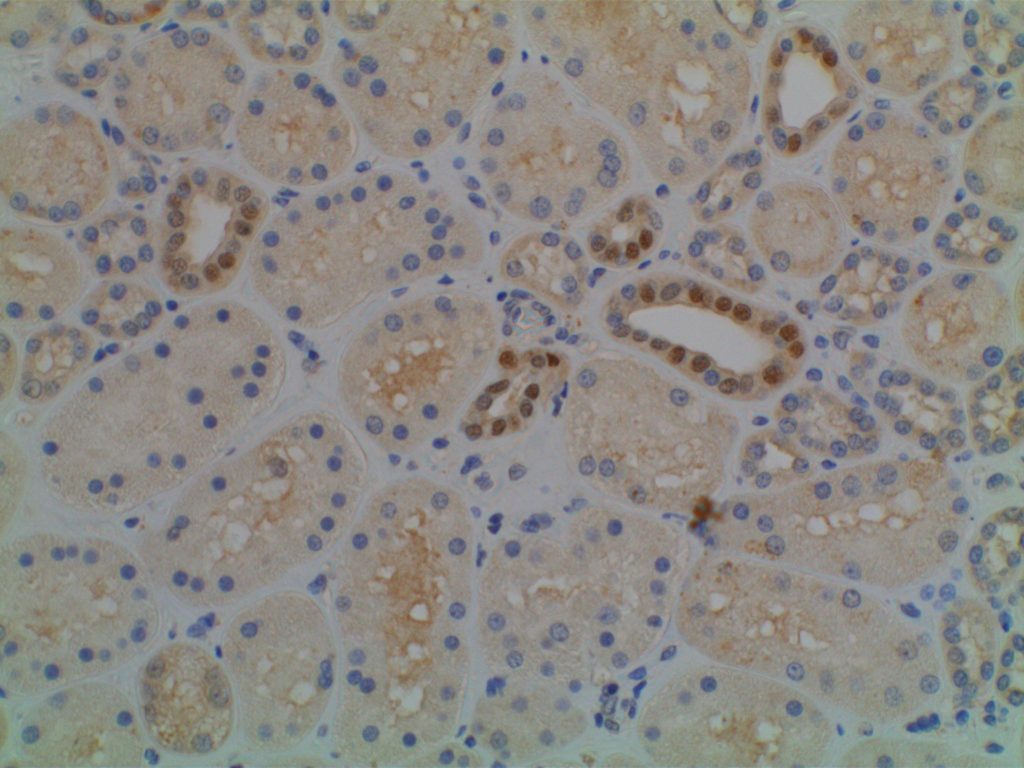
The expression pattern is nuclear, which is typically moderate to strong and diffuse. Some variability of the sensitivity of GATA-3 in breast carcinomas has been noted in the literature, and confirmation of one’s assay compared to the medical literature is recommended during the validation process. The following tables show data from multiple papers in the pathology literature.
Liu, et al (Biocare Medical, Concord, CA)
Tumor
GATA3
GCDFP15
MGB
Breast Carcinoma
94%
35-55%
65-70%
ER-negative breast ca.
69%
15%
35%
Urothelial Carcinoma
86%
Miettinen, et al (clone L50-823, dilution of 1:500; Biocare Medical, Concord, CA)
Tumor Type
%
N
Adrenocortical Carcinoma
11%
N=27
Basal Cell Ca., Skin
98%
N=62
Benign Skin Adnexal Tumors
100%
N=24
Breast, Ductal Ca., Primary
92%
N=179
Breast, Ductal Ca., Metastatic
96%
N=51
Breast, Lobular Carcinoma
100%
N=38
Malignant Mesothelioma
58%
N=64
Germ Cell Tumor, Choriocarcinoma
100%
N=11
Germ Cell Tumor, Endodermal Sinus Tumor
100%
N=6
Pancreas, Adenocarcinoma
37%
N=62
Renal Cell Carcinoma, Chromophobe
51%
N=35
Renal Oncocytoma
17%
N=35
Salivary Gland, Adenoid Cystic Carcinoma
29%
N=17
Salivary Gland, Ductal Carcinoma
43%
N=14
SCC – Skin
81%
N=31
SCC – Cervix
33%
N=21
SCC – Larynx
16%
N=36
SCC – Lung
12%
N=74
Urothelial Carcinoma – Low Grade
100%
N=22
Urothelial Carcinoma – High Grade
84%
N=32
No GATA-3 expression found in the following: Seminoma (n=76), Pure Embryonal Carcinoma (n=5), Lung Small Cell Carcinoma (n=30), Lung Carcinoid (n=11), Small Intestine Carcinoid (n=18), Merkel Cell Carcinoma (n=4), Ovary Non-Serous Carcinomas (n=25), Pancreatic Neuroendocrine Tumor, Rectal Adenocarcinoma (n=27), and Thymoma (n=41). (Miettinen, et al)
GATA-3 expression in 0-5% of tumors was found in the following: Stomach Adenocarcinoma (n=133), Thyroid Papillary and Follicular Carcinomas (n=75), Renal Cell Carcinoma NOT Chromophobe (n=154), Prostate Adenocarcinoma (n=95), Hepatocellular Carcinoma (n=47), and Colon Adenocarcinoma (n=142). (Miettinen, et al)
GATA-3 expression in 6-10% of tumors was found in the following: Anaplastic Thyroid Carcinoma (n=11), Ovarian Serous Carcinoma (n=73), Lung Adenocarcinoma (n=71), Cholangiocarcinoma (n=57), and Endometrial Adenocarcinoma (n=89). (Miettinen, et al)
Liu, et al. (GATA-3 [HG3-31]:sc-268; Santa Cruz Biotech, Santa Cruz, CA)
Tumor
%
N
Seminoma
0%
N=30
Embryonal Carcinoma
0%
N=24
Yolk Sac Tumor
0%
N=12
Lung Neuroendocrine Carcinoma
0%
N=61
Lung Adenocarcinoma
0%
N=61
Lung SCC
0%
N=49
Papillary Thyroid Carcinoma
0%
N=47
Follicular Thyroid Carcinoma
0%
N=37
Medullary Thyroid Carcinoma
0%
N=10
Clear Cell RCC
0%
N=82
Papillary RCC
0%
N=20
Colon Adenocarcinoma
0%
N=43
Esophageal Adenocarcinoma
0%
N=30
Gastric Adenocarcinoma
0%
N=21
Pancreatic Adenocarcinoma
0%
N=50
Urothelial Carcinoma
86%
N=72
Prostatic Adenocarcinoma
0%
N=136
Cholangiocarcinoma
0%
N=11
Breast Ductal Carcinoma
91%
N=99
Breast Lobular Carcinoma
100%
N=48
Endocervical Adenocarcinoma
0%
N=17
Endometrial Carcinoma
2%
N=96
Ovarian Serous Carcinoma
0%
N=56
Hepatocellular Carcinoma
0%
N=18
Pancreatic Endocrine Neoplasm
0%
N=15
Skin Melanoma
0%
N=100
Clark, et al.
Tumor
%
N
Breast
– HR+/Her2=
99%
N=131
– HR+/Her2+
100%
N=18
– HR=/Her2+
100%
N=7
– Triple Negative
73%
N=30
Endocervix
18%
N=34
Vulva/Cervix SCC
60%
N=10
Endometrium
7%
N=55
Ovary
10%
N=50
Bladder
95%
N=22
Liver (cholangiocarcinoma)
3%
N=62
Pancreas
10%
N=30
Stomach
2%
N=62
Parathyroid vs. Thyroid
GATA-3 has been shown to be expressed in >95% of parathyroid samples (n=25 combined) consisting of hyperplastic glands and adenomas, whereas no thyroid tissues showed GATA-3 expression.
Interestingly, IHC for PTH only stained between 1/3 and 2/3rds of parathyroid samples. Therefore, GATA-3 combined with TTF-1 may be very helpful in differentiating between thyroid and parathyroid lesions in small samples (e.g. thyroid FNAs). (Takada, et al.)
Photomicrographs
GATA-3 – BreastGATA-3 expression in a clear cell renal cell carcinomaGATA-3 expression in benign renal parenchyma.
References
Liu, H., Shi, J., Wilkerson, M. L., & Lin, F. (2012). Immunohistochemical evaluation of GATA3 expression in tumors and normal tissues: a useful immunomarker for breast and urothelial carcinomas. American Journal of Clinical Pathology, 138(1), 57–64. doi:10.1309/AJCP5UAFMSA9ZQBZ
Miettinen, M., McCue, P. A., Sarlomo-Rikala, M., Rys, J., Czapiewski, P., Wazny, K., et al. (2014). GATA3: A Multispecific But Potentially Useful Marker in Surgical Pathology: A Systematic Analysis of 2500 Epithelial and Nonepithelial Tumors. The American Journal of Surgical Pathology, 38(1), 13–22. doi:10.1097/PAS.0b013e3182a0218f
Ellis, C. L., Chang, A. G., Cimino-Mathews, A., Argani, P., Youssef, R. F., Kapur, P., et al. (2013). GATA-3 immunohistochemistry in the differential diagnosis of adenocarcinoma of the urinary bladder. The American Journal of Surgical Pathology, 37(11), 1756–1760. doi:10.1097/PAS.0b013e31829cdba7
Zhao, L., Antic, T., Witten, D., Paner, G. P., Taxy, J. B., Husain, A., et al. (2013). Is GATA3 expression maintained in regional metastases?: a study of paired primary and metastatic urothelial carcinomas. The American Journal of Surgical Pathology, 37(12), 1876–1881. doi:10.1097/PAS.0b013e31829e2525
Clark, B. Z., Beriwal, S., Dabbs, D. J., & Bhargava, R. (2014). Semiquantitative GATA-3 Immunoreactivity in Breast, Bladder, Gynecologic Tract, and Other Cytokeratin 7-Positive Carcinomas. American Journal of Clinical Pathology, 142(1), 64–71. doi:10.1309/AJCP8H2VBDSCIOBF
McCleskey BC, Penedo TL, Zhang K, Hameed O, Siegal GP, Wei S. GATA3 Expression in Advanced Breast Cancer: Prognostic Value and Organ-Specific Relapse. Am J Clin Pathol. 2015;144: 756–763.
doi:10.1309/AJCP5MMR1FJVVTPK
Takada, N., Hirokawa, M., Suzuki, A., Higuchi, M., Kuma, S., Miyauchi, A. (2016). Diagnostic value of GATA-3 in cytological identification of parathyroid tissues Endocrine Journal 63(7), 621-626. https://dx.doi.org/10.1507/endocrj.ej15-0700