CD30 (Ki-1 antigen) is a member of the tumor necrosis receptor factor family (TNRF) and is not a specific marker. CD30 will mark activated benign lymphoid cells in addition to several characteristic lymphoproliferative disease subtypes (e.g. Classical Hodgkin lymphoma and anapestic large cell lymphoma) of both B-cell and T-cell lineages.
CD30 Expression Pattern
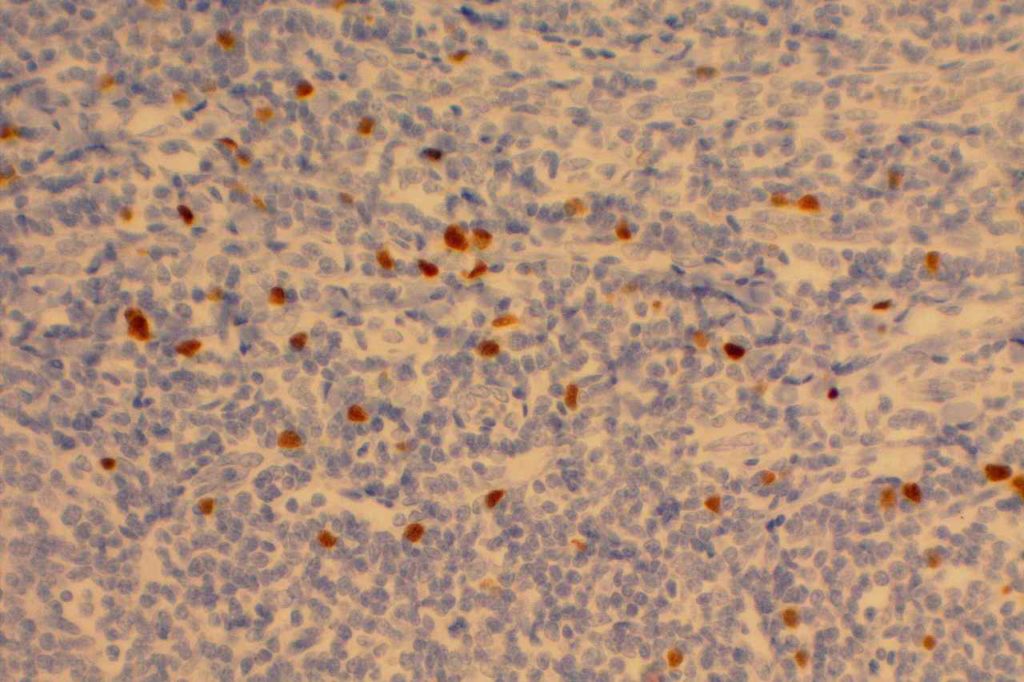
- Benign “Activated” lymphoid cells
- EBV-driven lymphoproliferative disorders and reactive proliferations (e.g. mononucleosis)
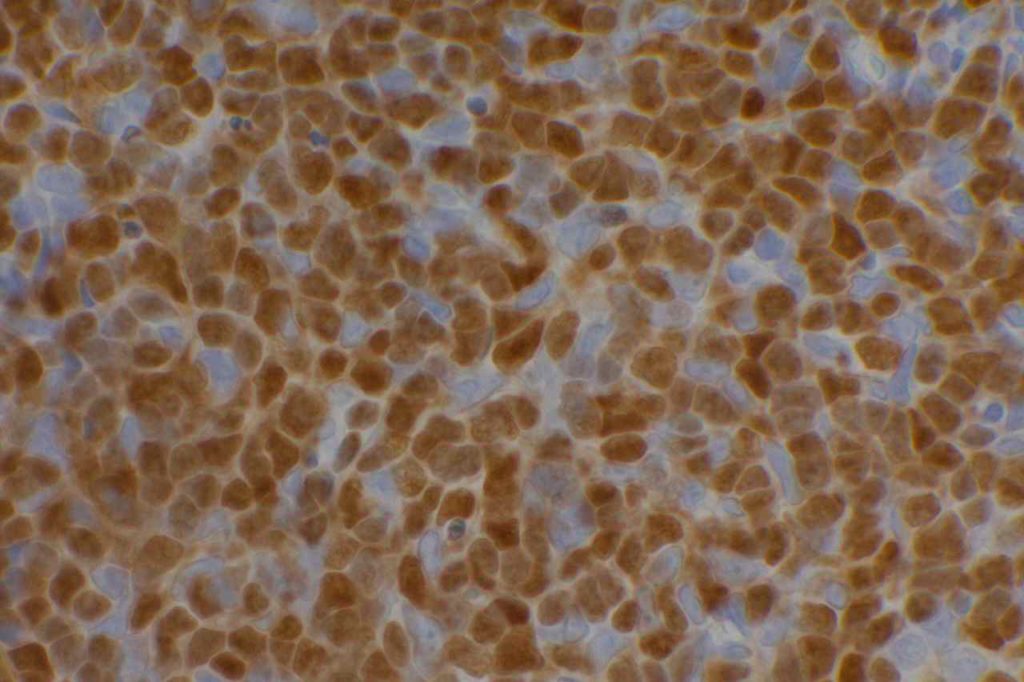
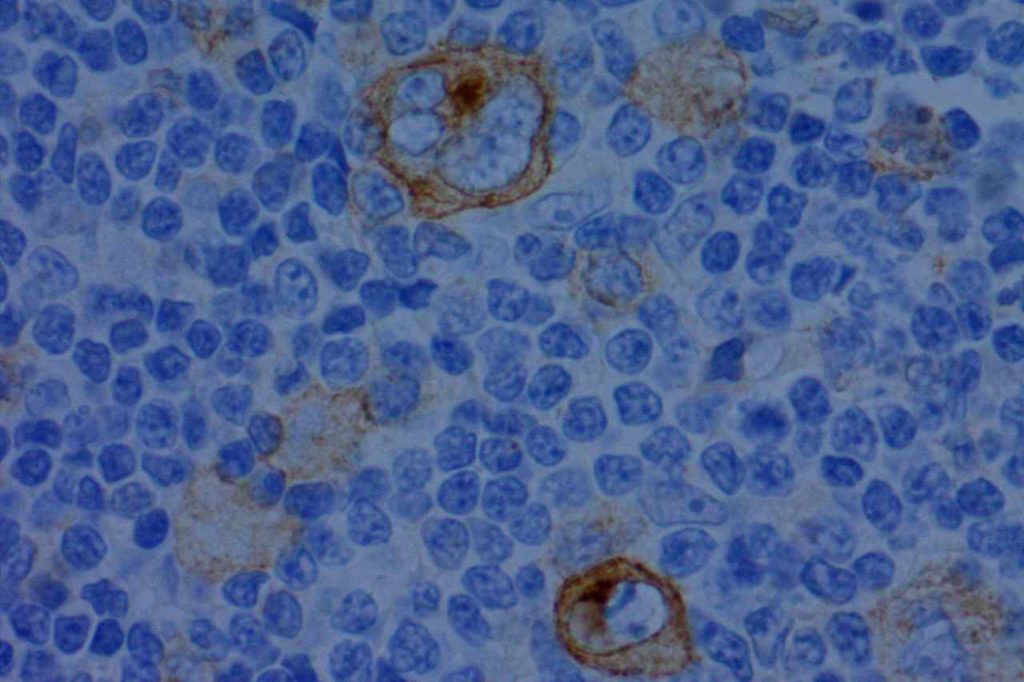
- Classical Hodgkin Lymphoma
- Anaplastic Large Cell Lymphoma (ALK+/ALK-)
- Peripheral T-cell Lymphomas (subset)
- Diffuse Large B-cell Lymphoma (subset)
- Primary Mediastinal Large B-Cell Lymphoma
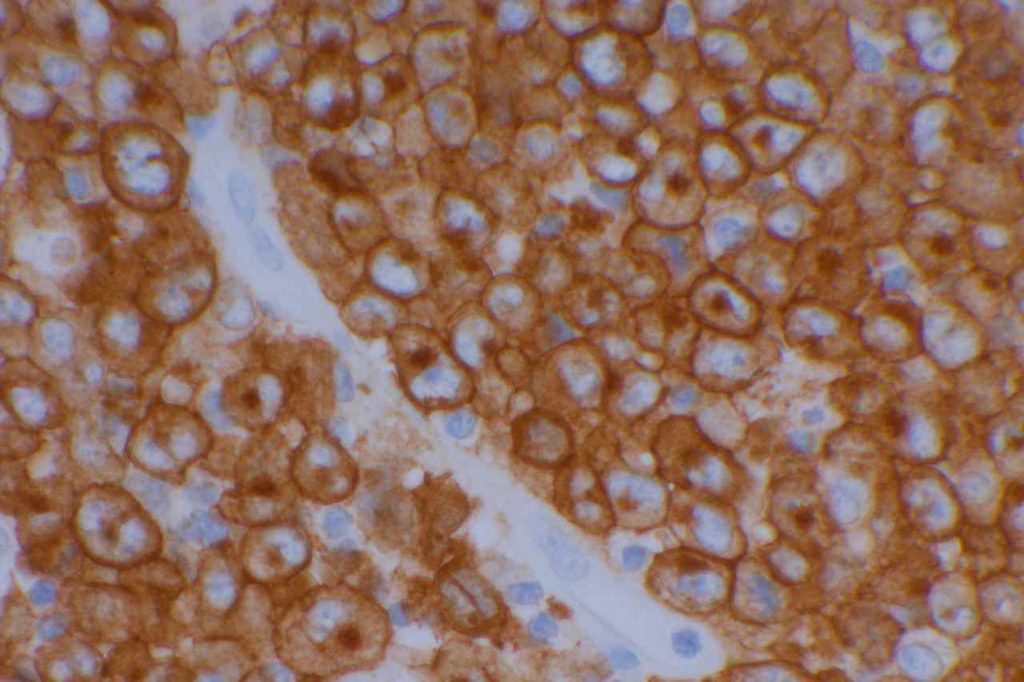
- Embryonal Carcinoma
- Germ Cell Tumors
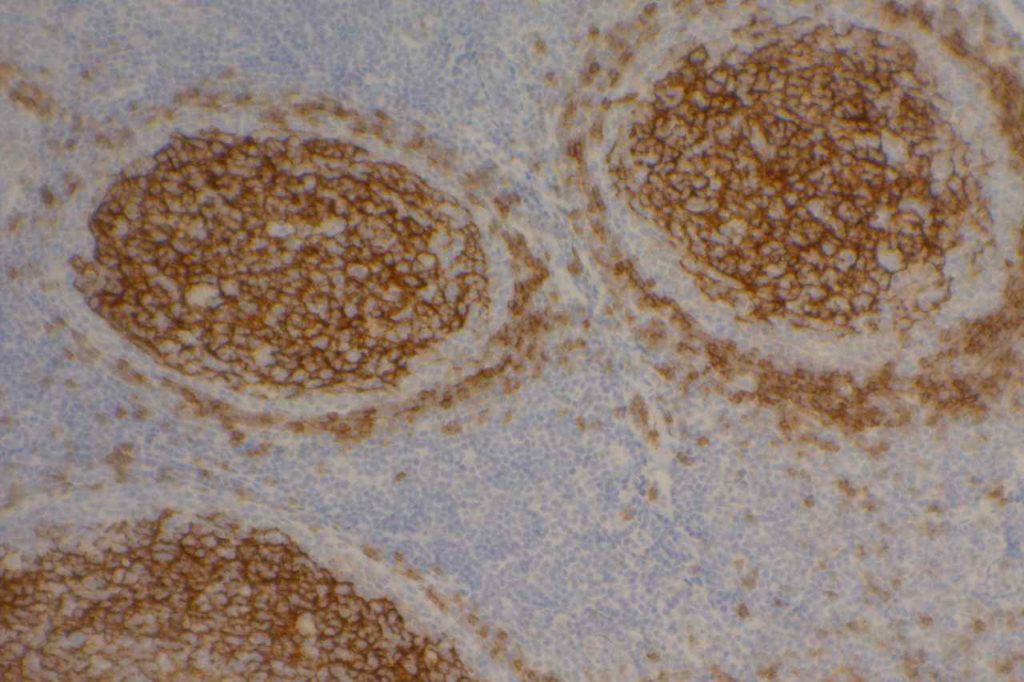
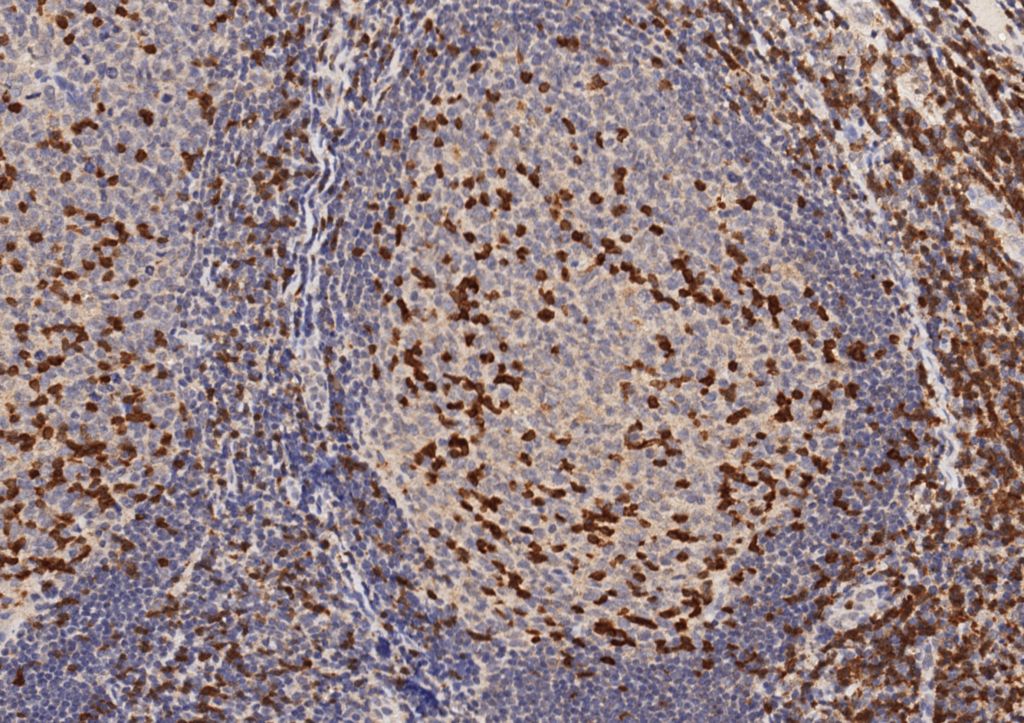
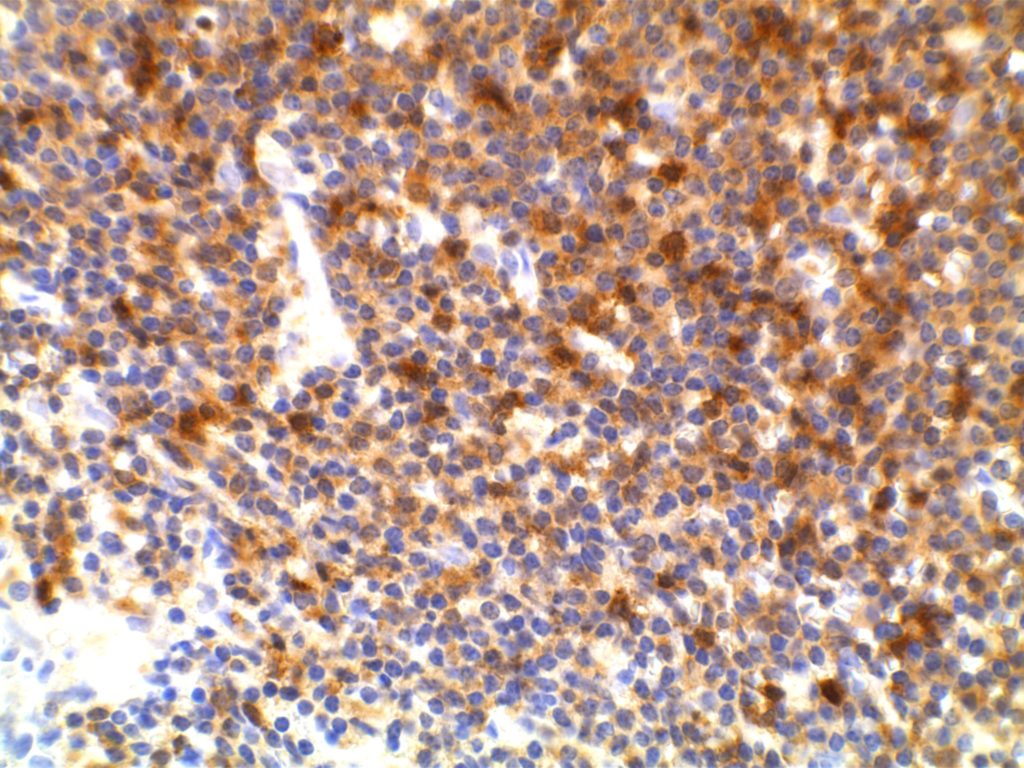
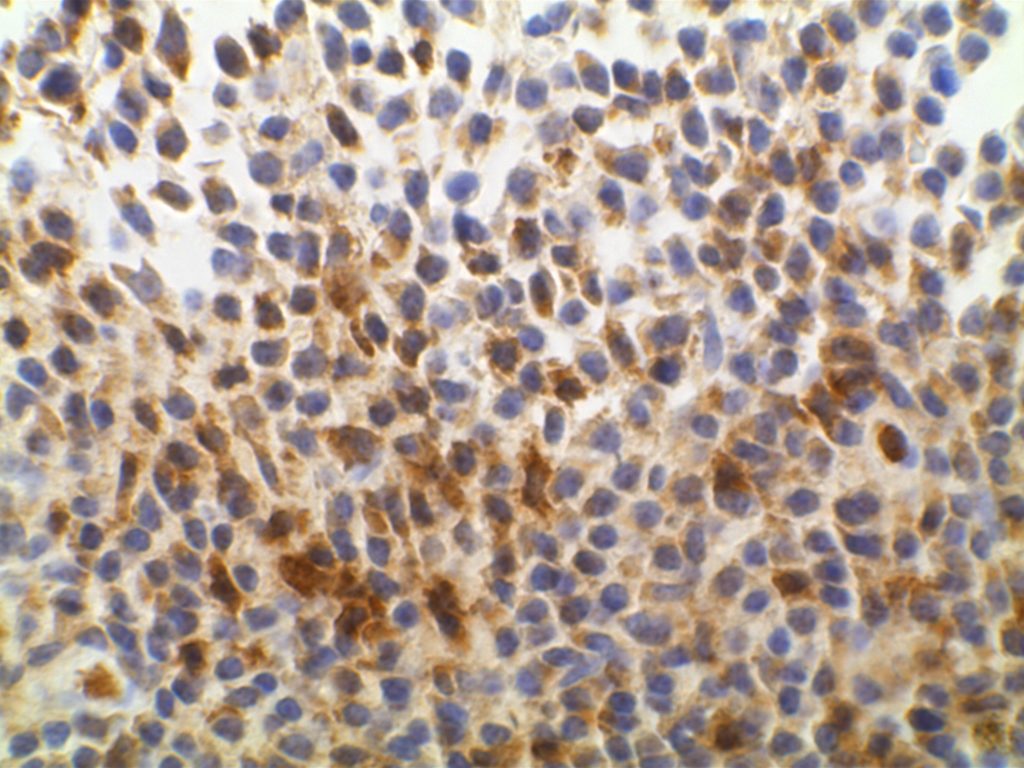
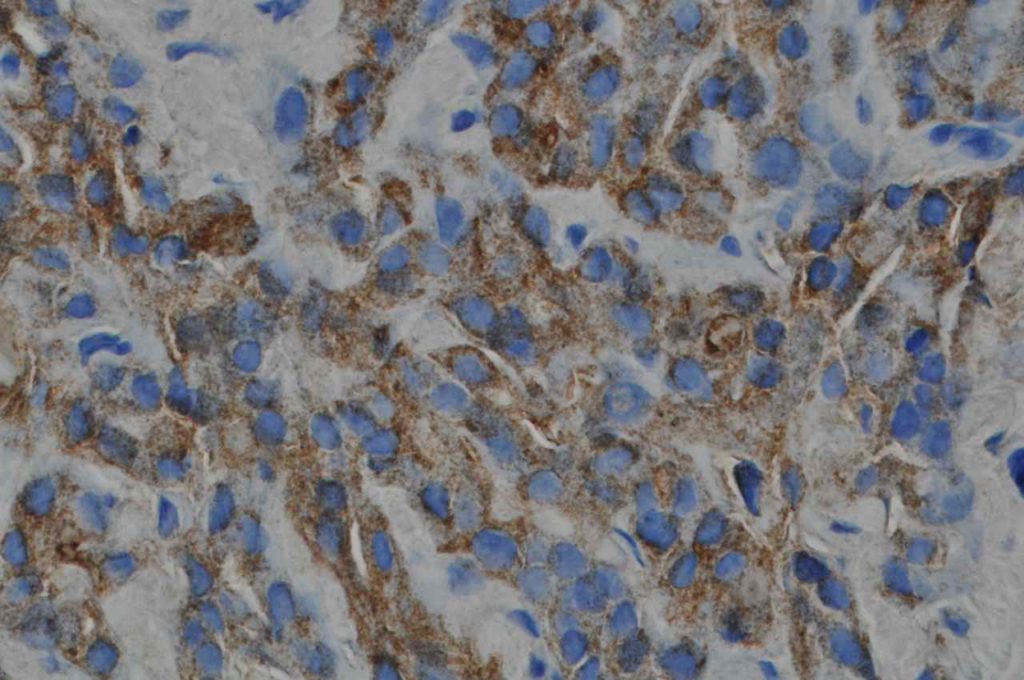
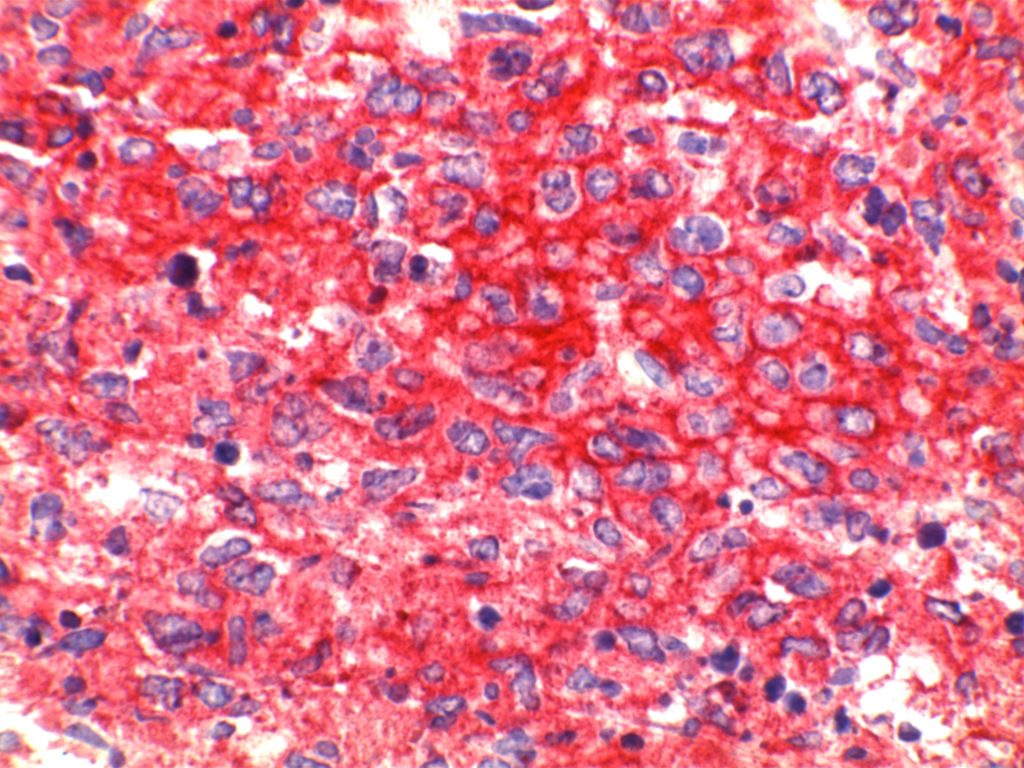
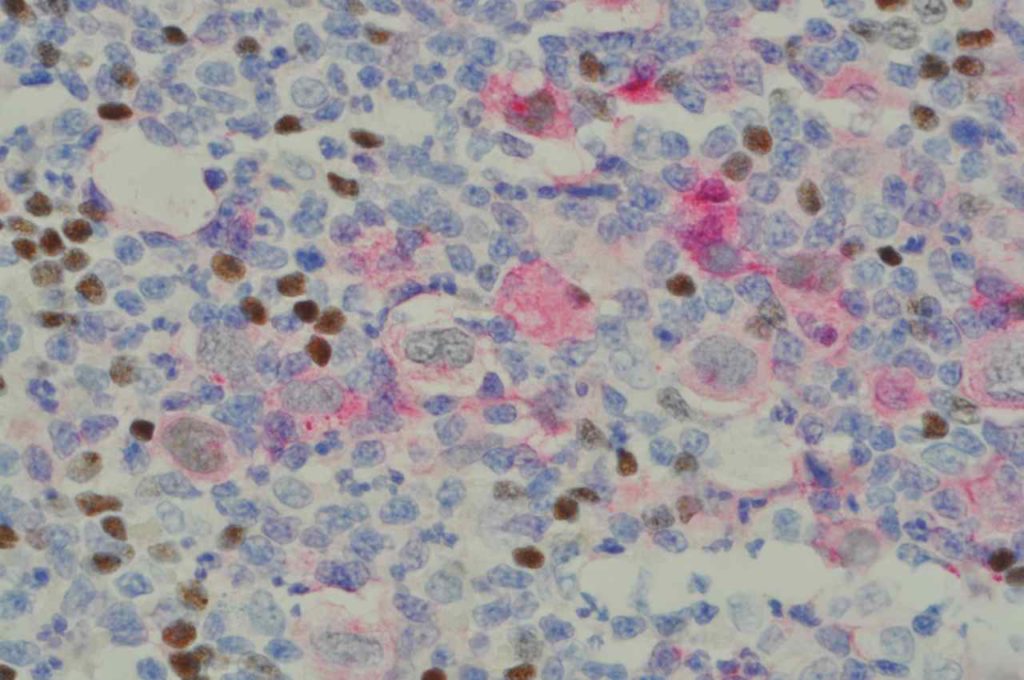
CD30 is an “activation” marker on T and B cells. This marker is most often used in the work-up of cases of Hodgkin lymphoma, anaplastic large cell lymphoma (ALCL), and embryonal carcinoma. The staining pattern has a membraneous and Golgi pattern. B5 fixative has negative impact on staining. CD30 is also helpful in the diagnosis of mediastinal large B cell lymphoma (focal/patchy and dim staining).
Unfortunately, CD30 lacks specificity, and in addition to the staining pattern in normal cells compartments, it may also be expressed in a variety of disease processes including: peripheral T-cell lymphoma (occasional), primary effusion lymphoma, cutaneous CD30+ lymphoproliferative disorders, DLBCL (variable, focal), plasmablastic lymphoma, sinonasal NK/T cell lymphoma, embryonal carcinoma of the testis (100%), Yolk sac tumors (24%), & mesothelioma (rare).
Nodular LP Hodgkin lymphoma, Adult T cell leukemia/lymphoma, pre B ALL, and systemic mastocytosis should not express CD30.
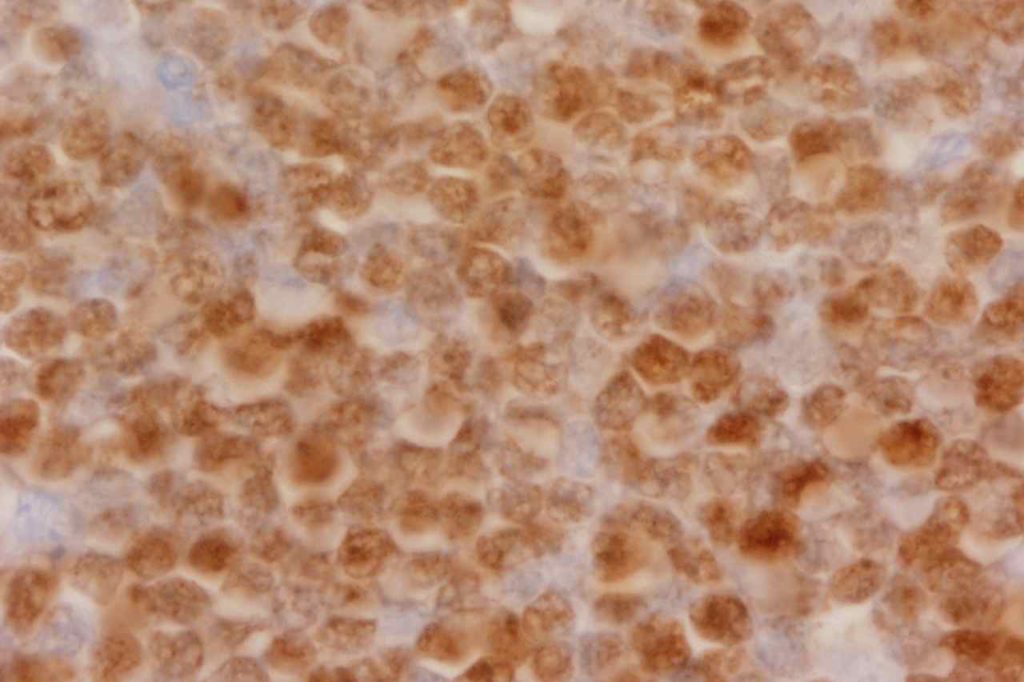
CD30+ DLBCL
Cases of DLBCL which co-express CD30 (~14%, n=903) had a more favorable 5-year survival (79% vs. 59%) in both germinal center and activated B-cell phenotypes. Gene expression profiling (GEP) revealed down regulation of proliferation and B-cell receptor signaling with up regulation of nuclear factor kappaB activation and lymphocyte survival. CD30+ EBV+ DLBCLis a unique subset of lymphomas with an aggressive clinical course. The WHO classification separates EBV+ cases into a separate category.
Clinical Significance
Brentuximab vedotin (Adcetris®) is an anti-CD30 monoclonal antibody used to treat anaplastic large cell lymphoma and relapsed or refractory Hodgkin lymphoma. Ongoing research with promise is active in other CD30 positive neoplastic processes.
References
Wick, MR. “Immunohistochemical approaches to the diagnosis of undifferentiated malignant tumor.”Annals of Diagnostic Pathology12(2008):72-84.
Bone Marrow IHC. Torlakovic, EE, et. al. American Society for Clinical Pathology Pathology Press © 2009. pp. 78-79.
Hu S, Xu-Monette ZY, Balasubramanyam A, Manyam GC, Visco C, Tzankov A, et al. CD30 expression defines a novel subgroup of diffuse large B-cell lymphoma with favorable prognosis and distinct gene expression signature: a report from the International DLBCL Rituximab-CHOP Consortium Program Study. Blood. 2013;121: 2715–2724. doi:10.1182/blood-2012-10-461848
Ansell SM. Brentuximab vedotin. Blood. 2014. doi:10.1182/blood-2014-06