Synaptophysin reacts with the integral membrane glycoprotein of presynaptic vesicles. It is less specific than chromogranin, and it may mark neurofilaments and epithelial filaments. Some neuroendocrine neoplasms will mark with synaptophysin and not chromogranin A. The converse can also be true. Therefore, chromogranin A and synaptophysin should be used in tandem to identify neuroendocrine differentiation (Wick, MR). CD56 is often considered the most sensitive neuroendocrine marker, but it is not as specific as chromogranin and synaptophysin (Bahrami, A, et al).
Neuroendocrine differentiation may not be readily recognized until it is revealed by immunohistochemistry, but may be important as these tumors may be responsive to similar therapy used for small cell carcinoma (Bahrami, A, et al).
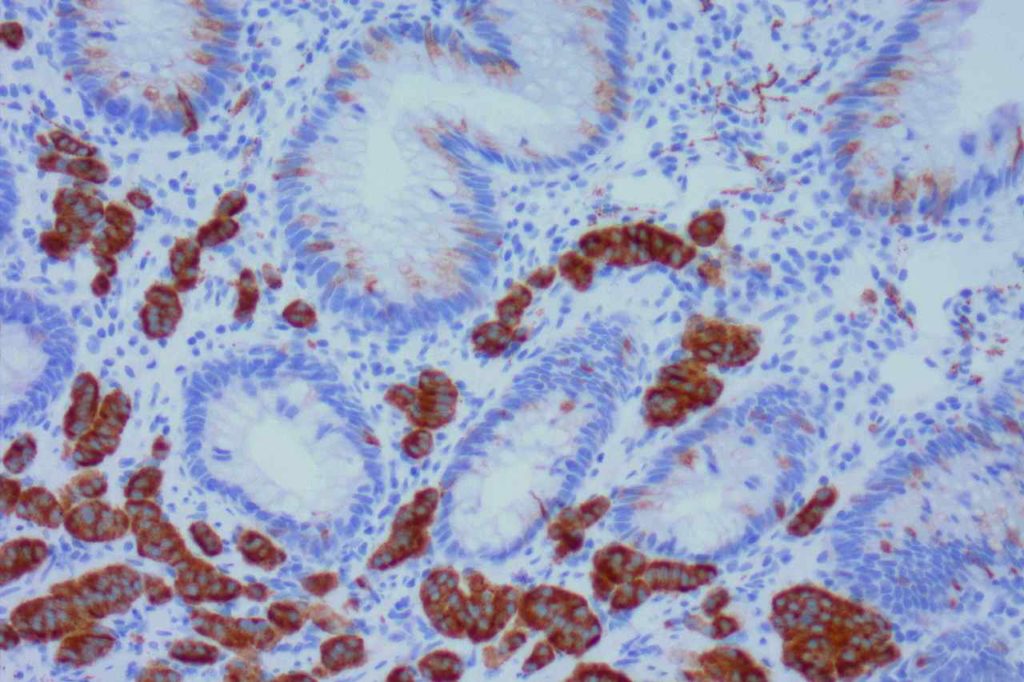
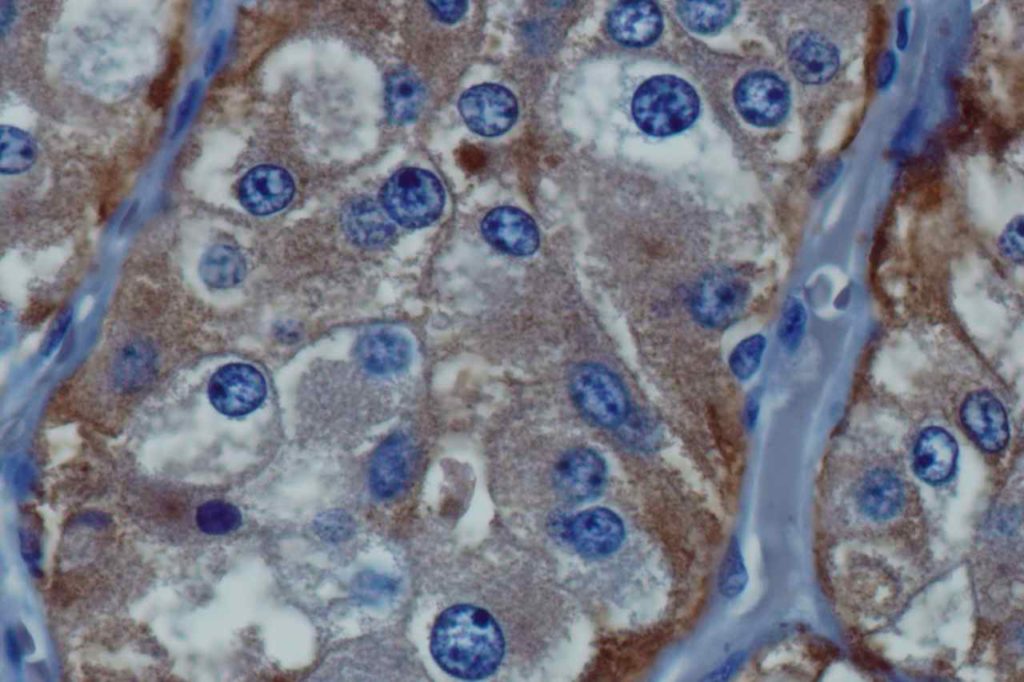
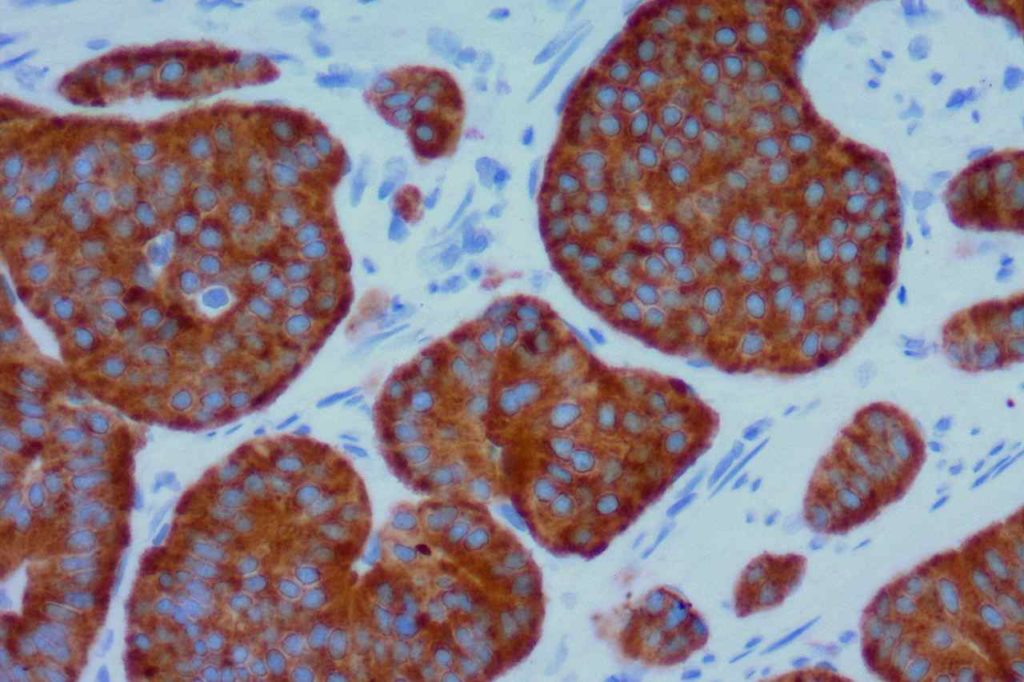
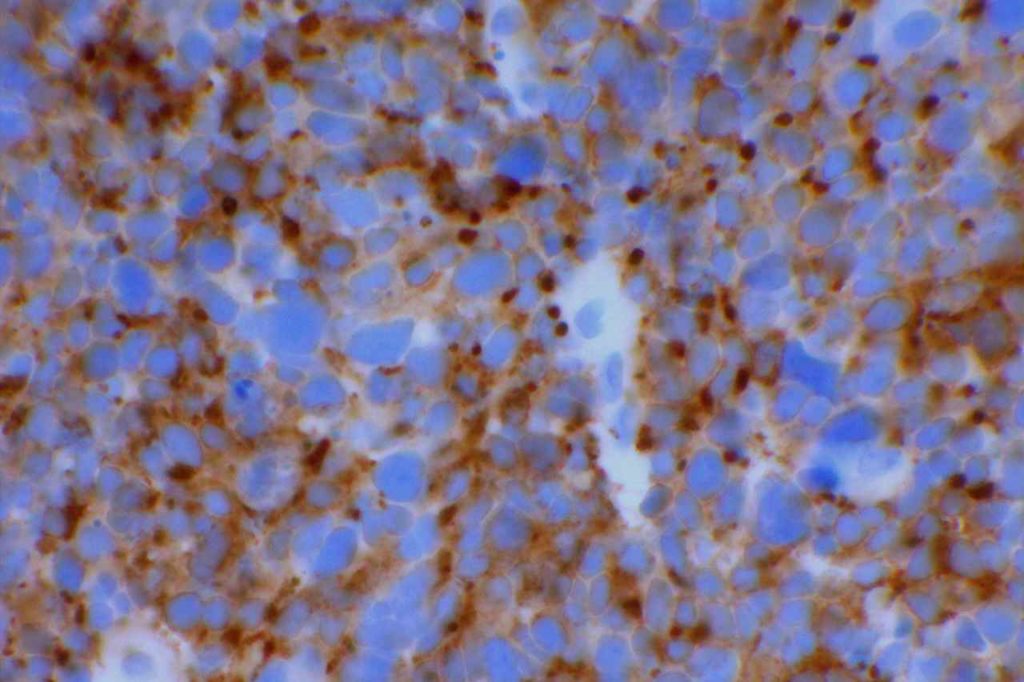
Microscopic Images
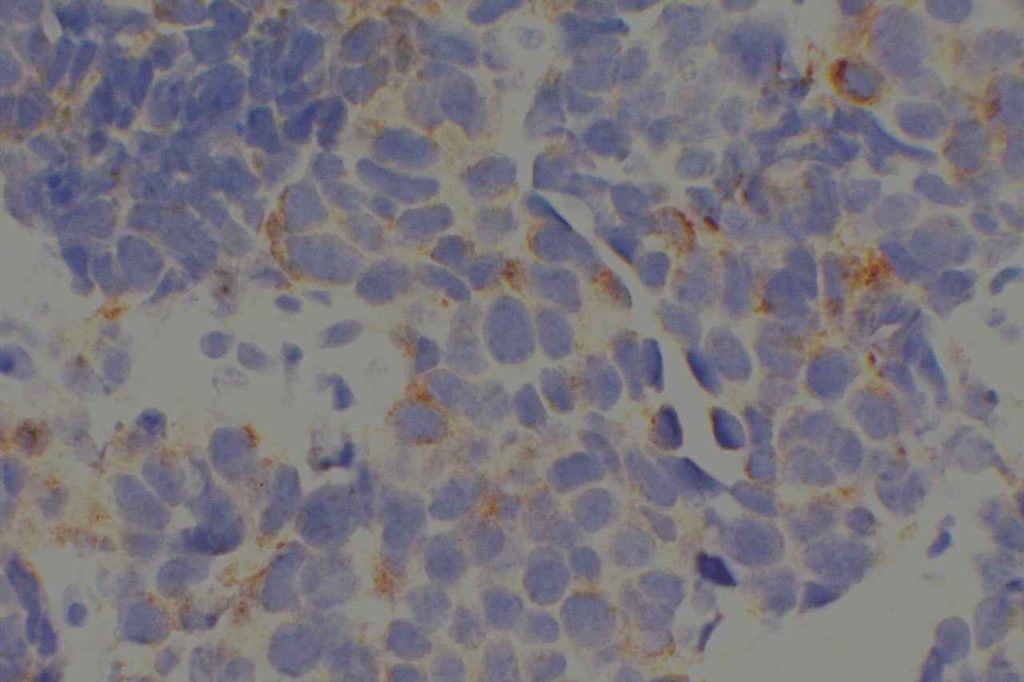
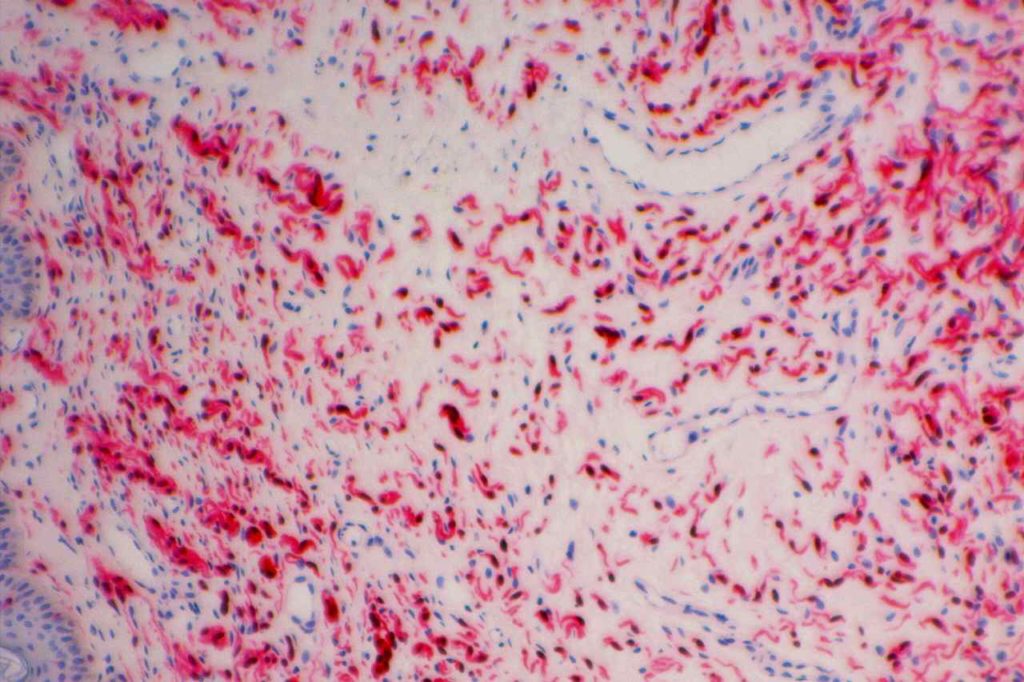
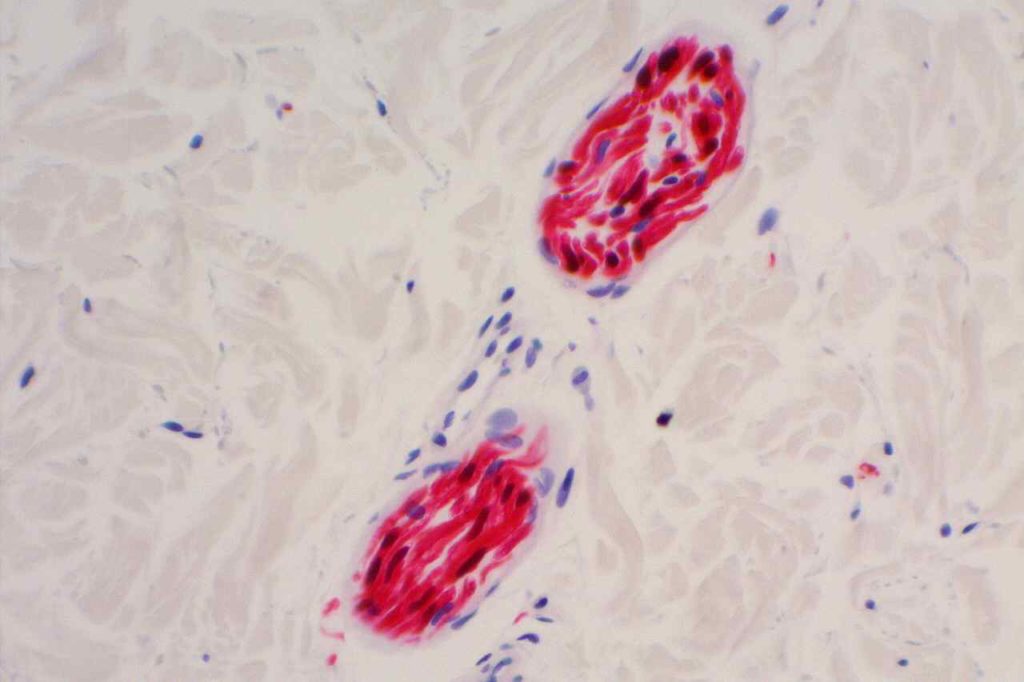
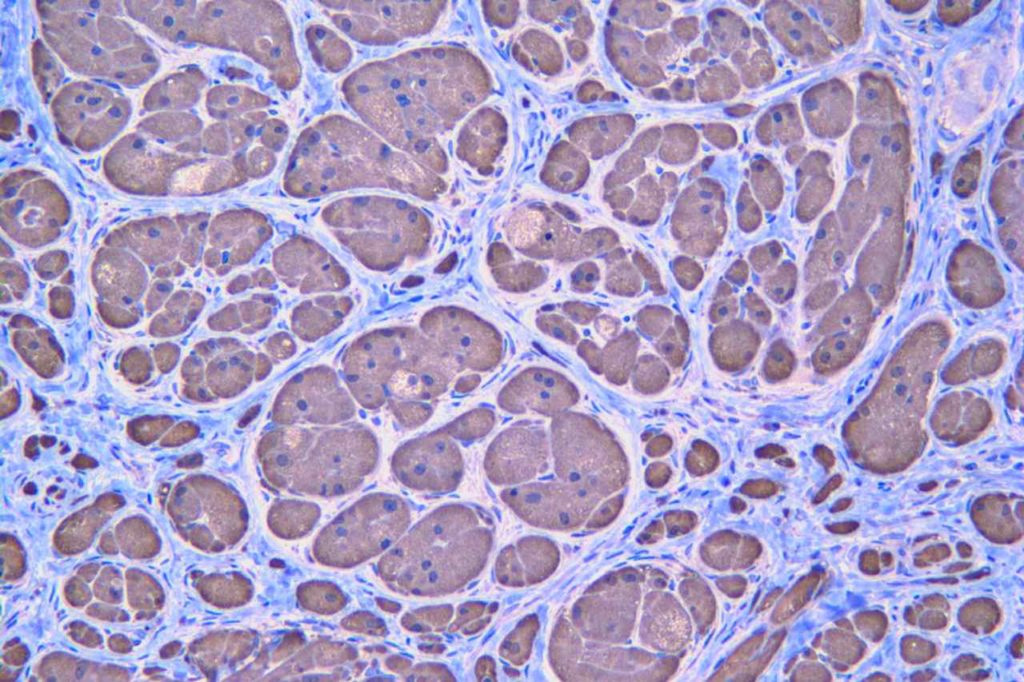
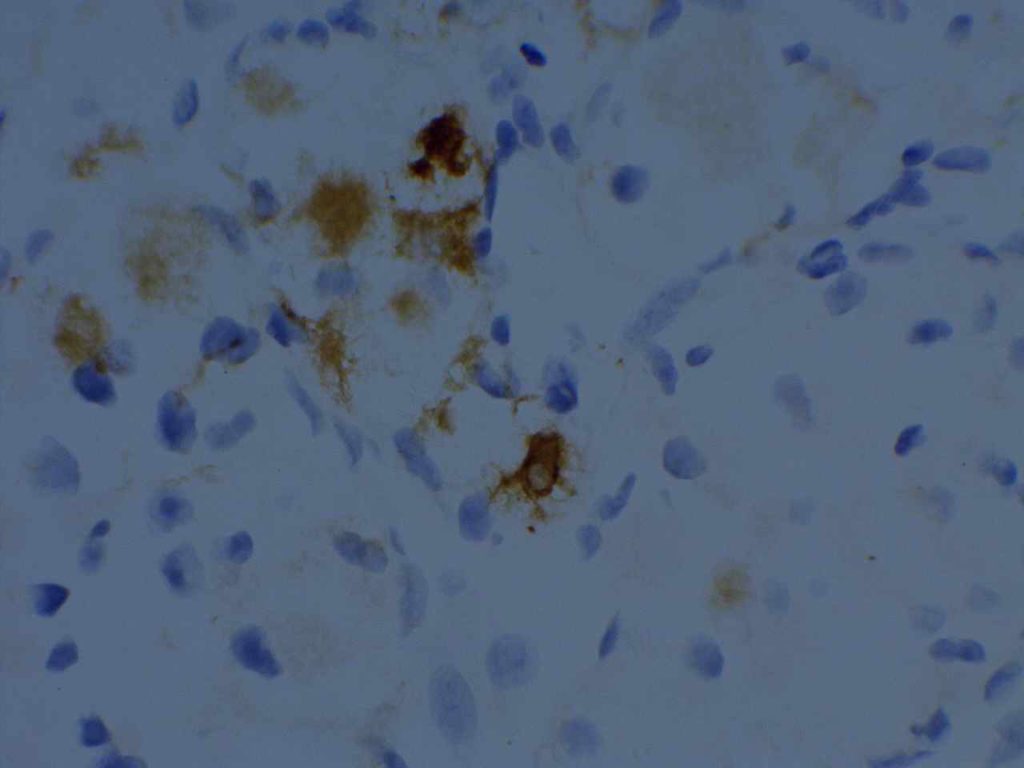
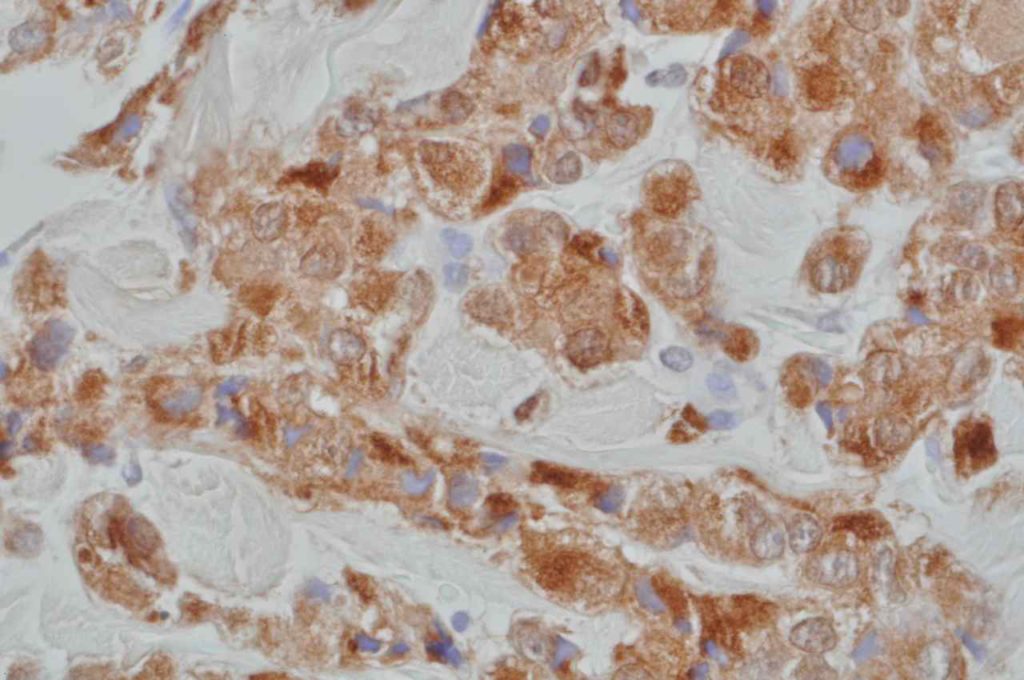
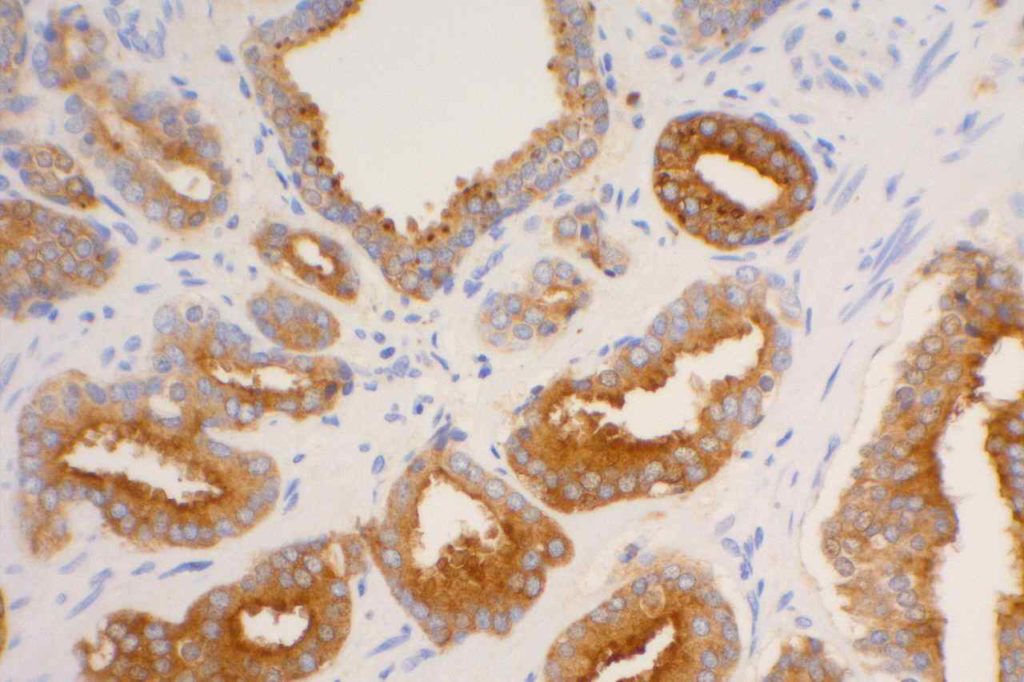
Synaptophysin expression in a gastric carcinoid.Synaptophysin expression in a pheochromocytoma.Synaptophysin expression in a carcinoid tumor.Synaptophysin expression in a Merkel cell carcinoma.Synaptophysin expression in a lung small cell carcinoma.
References
Wick, M. R. (2008). Immunohistochemical approaches to the diagnosis of undifferentiated malignant tumors. Annals of Diagnostic Pathology, 12(1), 72–84. doi:10.1016/j.anndiagpath.2007.10.003
Bahrami, A., Truong, L. D., & Ro, J. Y. (2008). Undifferentiated tumor: true identity by immunohistochemistry. Archives of Pathology & Laboratory Medicine, 132(3), 326–348.
SOX11 is a transcription factor found at chromosome 2p25.2, and is known to function in the development of the neural system. It is known to be expressed in normal adult squamous cells, certain lymphomas, and some ovarian carcinomas.
SOX10 (member of the SOX family of transcription factors and located at chromosome 22q13.1) is a transcription factor (Sry-related HMg-Box gene 10) protein, which functions as a nucleocytoplasmic shuttle protein, and is important in neural and melanocytic development. Expression has been identified in benign tissues (melanocytes, breast, ganglia, and optic vesicle) and in tumors (melanoma, malignant peripheral nerve sheath tumors, gliomas, breast carcinoma, and schwannoma).
Studies have shown SOX10 to be an excellent marker for melanoma (>95% sensitivity), but is not specific in differentiating nevi from melanoma as benign nevi/melanocytes also express SOX10. Specificity with respect to other tumor types appears relatively good with the exceptions described above. However, current data sets appear limited, and more study is needed to better define specificity.
SOX10 may be a helpful marker in the diagnosis of melanoma, especially when used with a panel of other markers like S-100, MART-1, or HMB-45. A head to head comparison with S-100 might be helpful to further characterize the antibodies usefulness as a screening tool for melanomas.
Expression of SOX10 is nuclear, as one would expect with transcription based markers.
In breast carcinoma, SOX10 is more commonly expressed in basal-like, triple negative, and metaplastic subtypes.
SOX10 Expression statistics using BC34 clone (Tacha, et. al)
Lesion
Percent +
Number
Melanoma (all subtypes)
92.6%
257
– Spindle Cell / Desmoplastic Melanoma
98%
51
Nevi
100%
20
Schwannomas
100%
28
Invasive Ductal (Breast) Carcinoma
16.5%
109
CNS Neoplasms
48%
52
– Astrocytomas
53%
41
Various Sarcomas
4%
99
Microscopic Images
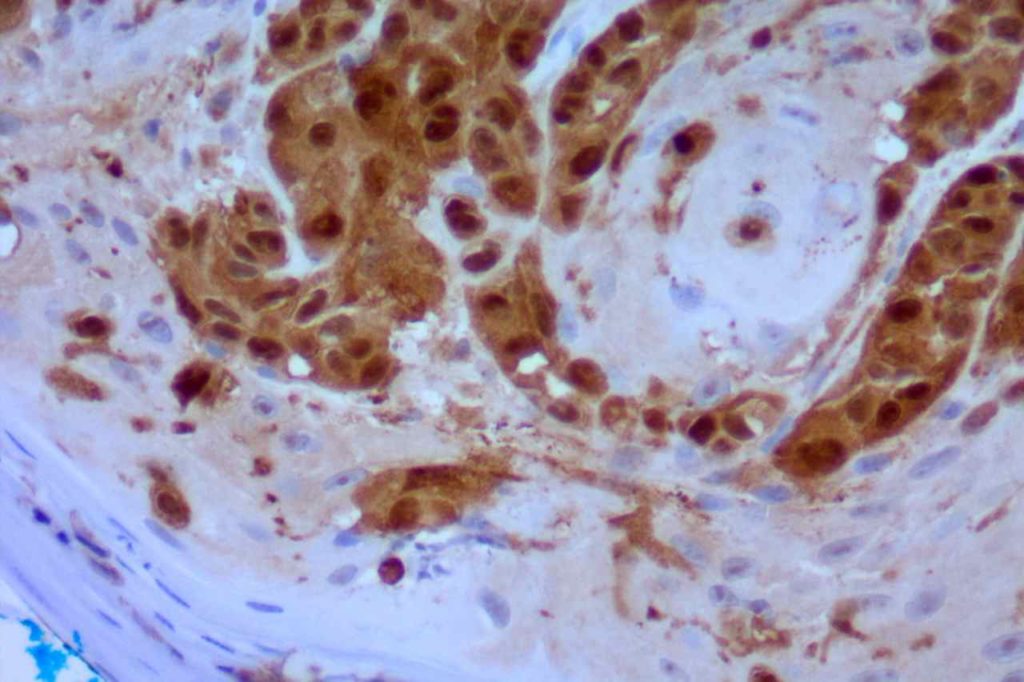
SOX10 highlighting scattered melanocytes in the skin epidermis.
References
Mohamed A, Gonzalez RS, Lawson D, Wang J, Cohen C. SOX10 expression in malignant melanoma, carcinoma, and normal tissues. Appl Immunohistochem Mol Morphol. 2013;21: 506–510. doi:10.1097/PAI.0b013e318279bc0a
Tacha D, Qi W, Ra S, Bremer R, Yu C, Chu J, et al. A Newly Developed Mouse Monoclonal SOX10 Antibody Is a Highly Sensitive and Specific Marker for Malignant Melanoma, Including Spindle Cell and Desmoplastic Melanomas. Arch Pathol Lab Med. 2015;139: 530–536. doi:10.5858/arpa.2014-0077-OA
Chiu, K., Ionescu, D. N. & Hayes, M. SOX10 expression in mammary invasive ductal carcinomas and benign breast tissue. Virchows Arch474, 667–672 (2019).
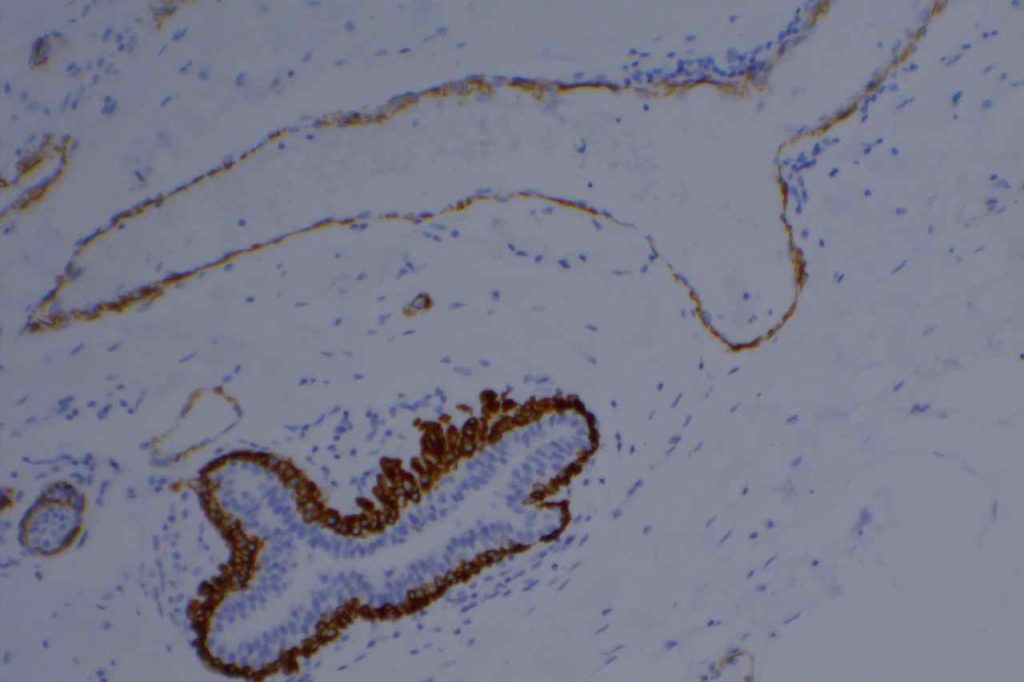
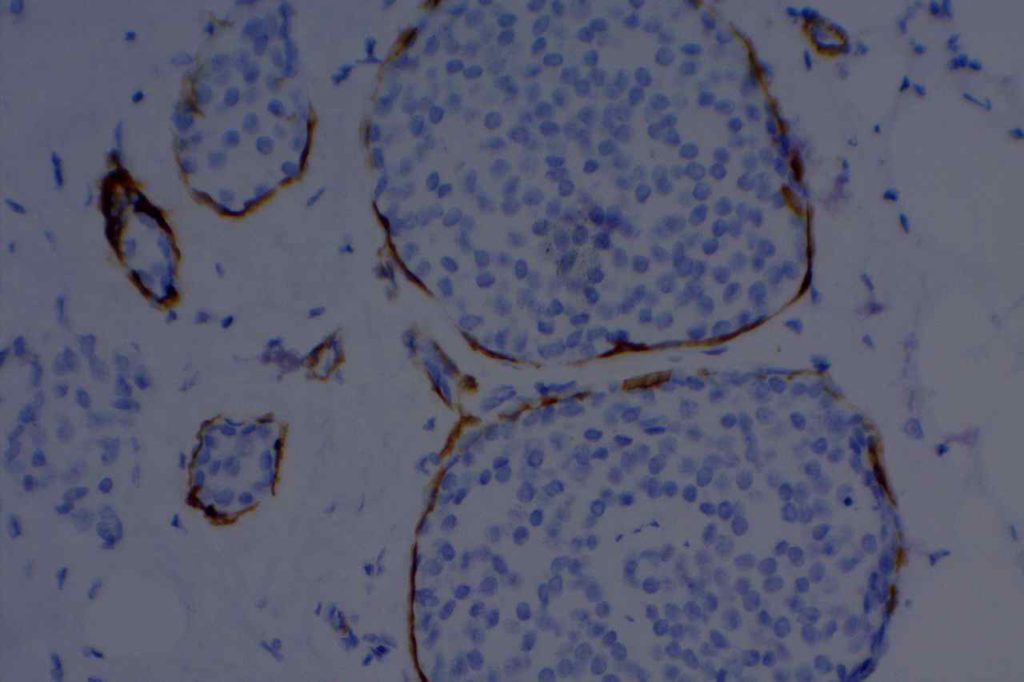
Smooth Muscle Myosin Heavy Chain (SMM-HC) is an antibody to the cytoplasmic structural protein, which is a component of the contractile apparatus in smooth muscle cells. SMM-HC is expressed in myoepithelial cells of the breast, which makes it a very useful stain in the differentiation of in situ and invasive lesions.
One of the big problems in the breast with smooth muscle markers is that myofibroblasts may have background expression, which can occasionally mimic myoepithelial cells. SMM-HC is one of the best markers (comparatively speaking) not to have a lot background expression in myofibroblasts. Calponin and smooth muscle actin have higher background staining of myofibroblasts.
SMM-HC is a more sensitive and specific marker in the differentiation of in situ and invasive breast carcinoma compared to CD10 [J Clin Pathol. 2007 Aug;60(8):958-9]. Another study noted that SMM-HC stained myofibroblasts in ~8% of cases compared to ~76% of cases for calponin. p63 is also a useful marker for breast myoepithelial cells, but the staining may not be as continuous as SMM-HC and occasional tumor cells may be positive for p63 (although the patter is recognizably different) [Am J Surg Pathol 2003 Jan;27(1):82-90]. SMM-HC combined with p63 as a dual stain may have synergistic and complementary effects.
Usefulness may be decreased in cases of DCIS, in which myoepithelial cells have been reported negative in up to 16% of DCIS cases (especially high grade DCIS). (Dewar, et al)
SMM-HC is also expressed in vascular smooth muscle cells.
Microscopic Images
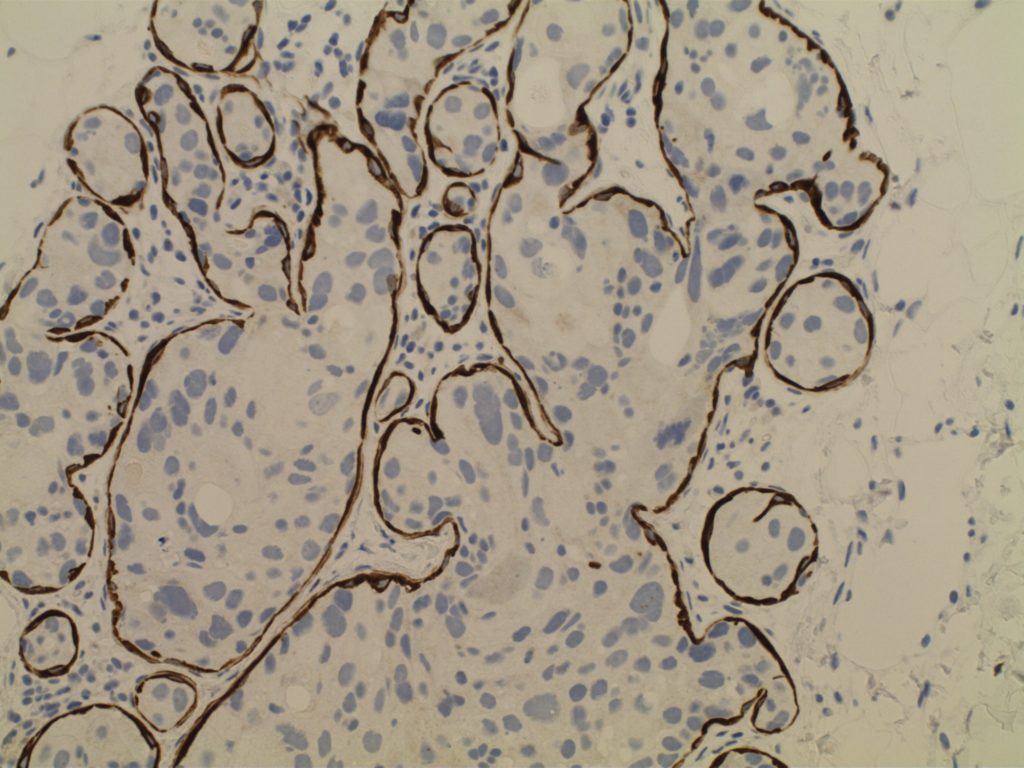
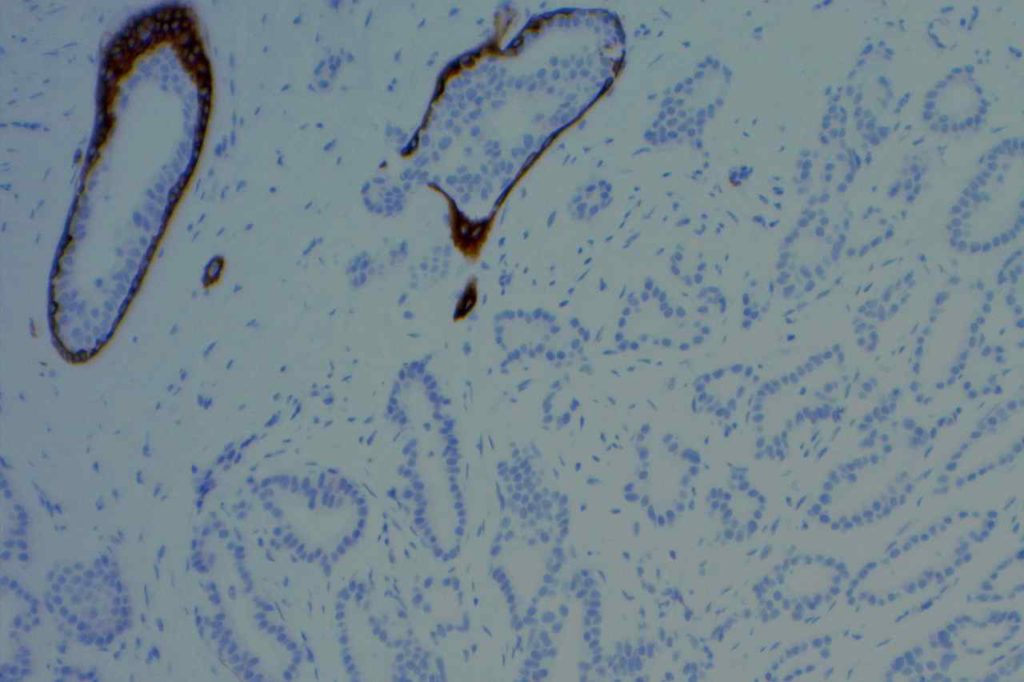
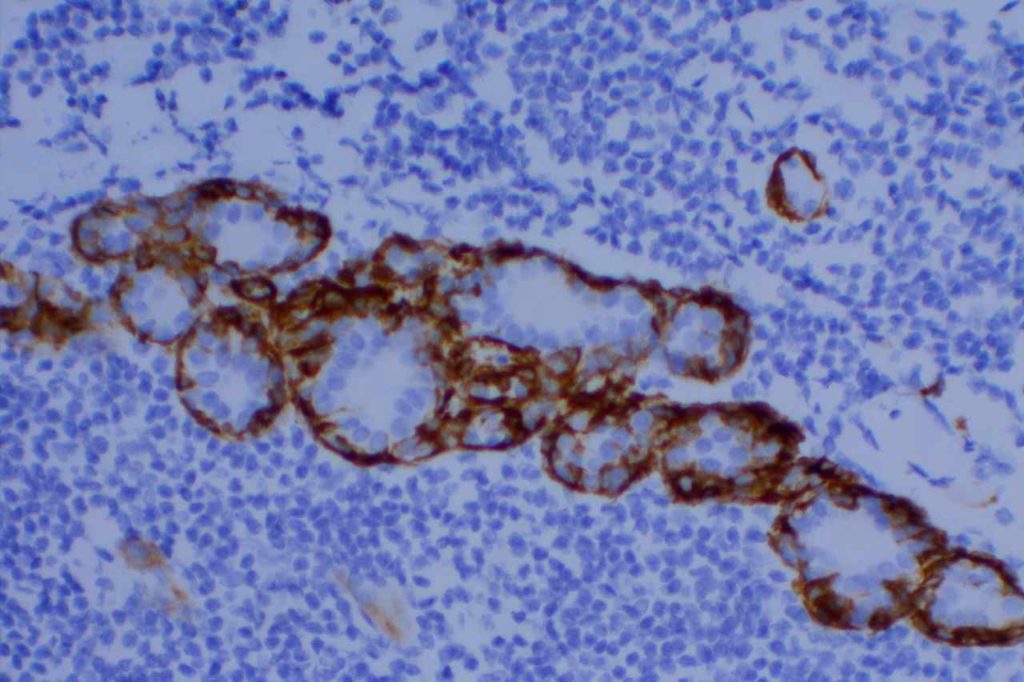
SMM-HC – High Grade DCIS. Intact myoepithelial cell layer highlighted by smooth muscle myosin-heavy chain.Smooth Muscle Myosin (SMM-HC) demonstrating loss of the myoepithelial cell layer in the invasive component.SMM-HC highlighting the myoepithelial layer in benign breast epithelium.SMM-HC highlighting vascular smooth muscle and benign duct structures.SMM-HC highlighting expanded duct structures.
References
Kalof AN, et. al. “Immunostaining patterns of myoepithelial cells in breast lesions: a comparison of CD10 and smooth muscle myosin heavy chain.” J Clin Pathol. 2004 vol. 57(6) pp. 625-629. doi:10.1136/jcp.2003.013227
Werling RW, et. al. “Immunohistochemical distinction of invasive from noninvasive breast lesions: a comparative study of p63 versus calponin and smooth muscle myosin heavy chain.” Am J Surg Pathol 2003 Jan;27(1):82-90.
Dewar, R., Fadare, O., Gilmore, H., & Gown, A. M. (2011). Best practices in diagnostic immunohistochemistry: myoepithelial markers in breast pathology. Archives of pathology & laboratory medicine, 135(4), 422–429. doi:10.1043/2010-0336-CP.1
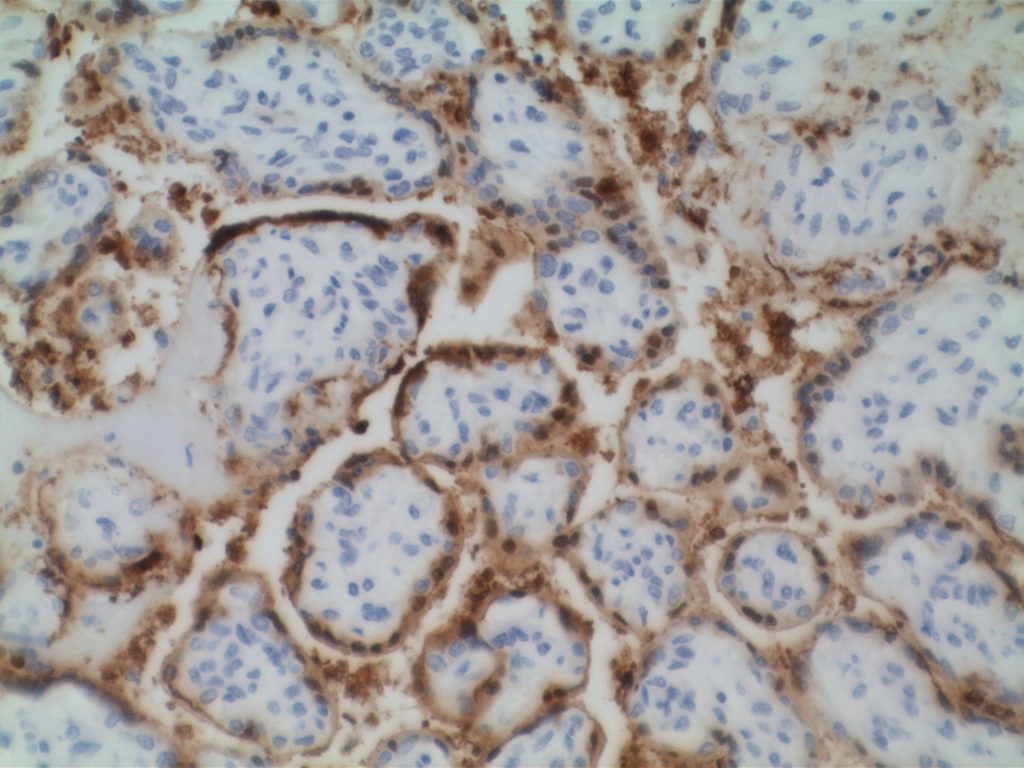
S100P (placental S100) is a member of the S100 family. It has been identified in human placenta and is expressed in a multitude of cancer types including: bladder, breast, esophagus, colon, lung, pancreatic, ovarian, hepatocellular (HCC), cholangiocarcinoma, and prostate (Yuan et al.). Interesting, Mohanty, et al. found S100P to be a relatively sensitive and specific marker for urothelial carcinoma in the differential of urothelial carcinoma vs. poorly differentiated prostate adenocarcinoma of the bladder neck (88% sensitive, 100% specific, N=16).
Practically, S100P may have some useful benefit in a limited differential setting, but given its general lack of specificity would probably not be significantly helpful in the setting of a large differential diagnosis.
Yuan, et al. did find S100P expression to be an independent poor prognostic indicator in HCC with early tumor recurrence or high tumor stage.
Microscopic Images
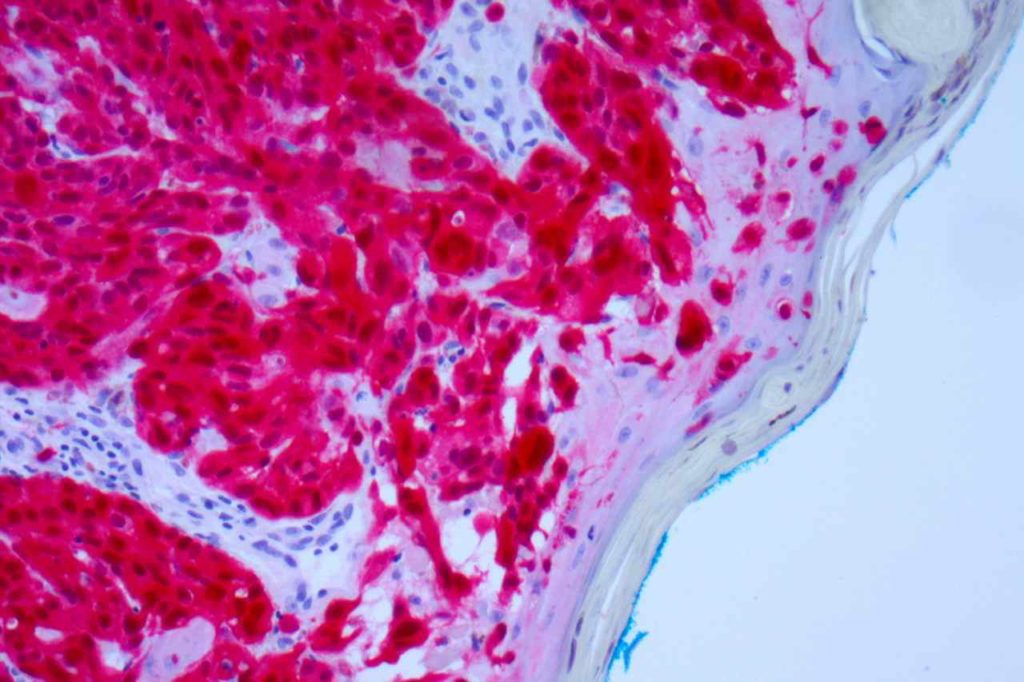
S100P expression in placental tissue (good control)S100P expression in metastatic prostate adenocarcinoma.
References
Yuan, R.-H., Chang, K.-T., Chen, Y.-L., Hsu, H.-C., Lee, P.-H., Lai, P.-L., & Jeng, Y.-M. (2013). S100P expression is a novel prognostic factor in hepatocellular carcinoma and predicts survival in patients with high tumor stage or early recurrent tumors. PloS One, 8(6), e65501. doi:10.1371/journal.pone.0065501
Mohanty SK, Smith SC, Chang E, et al. Evaluation of contemporary prostate and urothelial lineage biomarkers in a consecutive cohort of poorly differentiated bladder neck carcinomas. Am J Clin Pathol. 2014;142(2):173–183. doi:10.1309/AJCPK1OV6IMNPFGL.
S-100 is a marker that is most commonly used to identify cells of neural origin, including melanocytes and melanoma. S-100 is an antibody to the calcium-flux determinant protein, which is expressed by many different tissue types including: melanocytes, Schwann cells (nerve fibers), neural elements (astrocytes, ependyma, and oligodendroglia), Langerhans histiocytes, myoepithelial cells, reticulum cells, and salivary gland. Unfortunately, this variability of specificity can make the use of the S-100 antibody in isolation “risky business.” In fact, some carcinomas may express S-100. Therefore, in the work-up of a poorly differentiated lesion, it should be part of a larger panel.
S-100 expression can be nuclear and cytoplasmic.
Melanoma
S-100 is generally considered the most sensitive marker for melanoma (a few may argue vimentin), but has limitations in evaluation of lymph node tissue due to all of the background expression in dendritic cells. MART-1 (Melan A) and HMB-45 are typically used more commonly in these situations. As a general rule of thumb, the more epithelioid the melanoma, the more likely it will be to express MART-1 and HMB-45. As melanomas become more “spindled” the less they tend to express HMB-45 and MART-1. S-100 tends to retain expression in melanomas better as the pattern becomes more spindled compared to HMB-45 and MART-1
S-100 expression in nevus.S-100 expression in nerve fiber.S-100 expression in melanoma (DAB).S-100 expression in a malignant melanoma.S-100 expression in a granular cell tumor.
References
Wick, M. R. (2008). Immunohistochemical approaches to the diagnosis of undifferentiated malignant tumors. Annals of Diagnostic Pathology, 12(1), 72–84. doi:10.1016/j.anndiagpath.2007.10.003
Kucher, C., Zhang, P. J., Acs, G., Roberts, S., & Xu, X. (2006). Can Melan-A replace S-100 and HMB-45 in the evaluation of sentinel lymph nodes from patients with malignant melanoma? Applied Immunohistochemistry & Molecular Morphology : AIMM / Official Publication of the Society for Applied Immunohistochemistry, 14(3), 324–327.
Renal Cell Carcinoma Marker (RCC Ma) is a cytoplasmic marker that stains the renal proximal tubule brush border antigen. The following table (McGregor, et al) shows the stain sensitivity (>10% tumor cell staining):
Tumor Type
Sensitivity
RCC Clear Cell
84%
RCC Papillary
96%
RCC Chromophobe
45%
RCC Sarcomatoid
25%
Collecting Duct Carcinoma
0%
Oncocytoma
0%
Sharma, S.G., et. al. (PAX-2 and RCCma expression in various papillary tumors)
Tumor Type
No.
PAX2
RCCma
Papillary RCC
24
67%
96%
Ovarian Papillary Serous Carcinoma
10
40%
80%
Uterine Papillary Serous Carcinoma
9
56%
44%
Papillary Thyroid Carcinoma
9
0%
100%
Papillary Urothelial Carcinoma
10
0%
10%
Intraductal Papillary Mucinous Tumor of the Pancreas
2
0%
50%
Chroroid Plexus Papilloma
1
0%
100%
Pituitary Adenoma with Papillary Features
1
0%
100%
Lung Adenocarcinoma with Papillary Features
2
0%
50%
RCC Ma has been shown to be relatively specific for RCC in the metastatic setting, but is known to stain cells of other histogenesis (e.g. breast carcinoma, embryonal carcinoma, parathyroid adenomas, etc.). RCC Ma is a useful marker, but not recommended to be used in isolation (especially papillary lesions). It is also important to confirm the performance of this antibody within one’s laboratory because it has shown performance variability from laboratory to laboratory (author’s experience). A useful panel for renal cell carcinoma includes CD10, vimentin, AE1/AE3, and RCC Ma.
McGregor, D. K., Khurana, K. K., Cao, C., Tsao, C. C., Ayala, G., Krishnan, B., et al. (2001). Diagnosing primary and metastatic renal cell carcinoma: the use of the monoclonal antibody ‘Renal Cell Carcinoma Marker’. The American Journal of Surgical Pathology, 25(12), 1485–1492.
Sharma, S. G., Gokden, M., McKenney, J. K., Phan, D. C., Cox, R. M., Kelly, T., & Gokden, N. (2010). The utility of PAX-2 and renal cell carcinoma marker immunohistochemistry in distinguishing papillary renal cell carcinoma from nonrenal cell neoplasms with papillary features. Applied Immunohistochemistry & Molecular Morphology : AIMM / Official Publication of the Society for Applied Immunohistochemistry, 18(6), 494–498. doi:10.1097/PAI.0b013e3181e78ff8
Pan, Z., Grizzle, W., & Hameed, O. (2013). Significant variation of immunohistochemical marker expression in paired primary and metastatic clear cell renal cell carcinomas. American Journal of Clinical Pathology, 140(3), 410–418. doi:10.1309/AJCP8DMPEIMVH6YP
Zhai, Q. J. (2010). Application of Immunohistochemistry to the Diagnosis of Kidney Tumors. Pathology Case Reviews, 15(1), 25–34. doi:10.1097/PCR.0b013e3181d51c70
Prostate Specific Antigen (PSA) is a marker used to identify tumors of prostate epithelium origin. It is generally considered to be >95% sensitive for prostate carcinoma, and has better specificity that PSAP. However, as the Gleason score increases, the sensitivity decreases. This is important because it is not usually the well-differentiated tumors that cause diagnostic confusion, but the poorly differentiated ones. In an article by Mohanty, PSA expression was in the range of 25% for poorly differentiated prostate carcinomas present in the bladder trigone area, but an article by Goldstein indicates the sensitivity may be closer to 50% in high Gleason score tumors.
Common expression patterns in carcinoma [Clin Cancer Res 2005;11(10) May 15, 2005]
Tumor
Expression (%)
Breast
0%
Colon
0%
Lung
<10%
Ovary
0%
Pancreas
0%
Stomach
<5%
Prostate
>95%
PSA expression and other markers as a function of Gleason score (Goldstein, NS)
Gleason Score
PSA
CK7
CK20
PAP
6 (N=25)
100%
0%
0%
100%
7 (N=50)
98%
0%
2%
100%
8 (N=54)
56%
0%
4%
65%
9 (N=58)
52%
10%
16%
74%
10 (N=38)
47%
13%
26%
61%
Prostate specific antigen (PSA), Prostatic acid phosphatase (PAP). Reactivity was defined as >25% positive cells.
Microscopic Images
PSA expression in prostate adenocarcinoma.PSA expression in prostate.PSA expression in prostate adenocarcinoma.PSAP expression in prostate gland tissue (adenocarcinoma).
References
Goldstein NS. Immunophenotypic characterization of 225 prostate adenocarcinomas with intermediate or high Gleason scores. Am J Clin Pathol. 2002;117(3):471–477. doi:10.1309/G6PR-Y774-X738-FG2K.
Mohanty SK, Smith SC, Chang E, et al. Evaluation of contemporary prostate and urothelial lineage biomarkers in a consecutive cohort of poorly differentiated bladder neck carcinomas. Am J Clin Pathol. 2014;142(2):173–183. doi:10.1309/AJCPK1OV6IMNPFGL.
Prostate-specific membrane antigen (PSMA) is a glycoprotein, which functions as folate hydrolase, and is very specific for prostate tissue (benign and malignant). Expression can be seen with various patterns including: cytoplasmic and membraneous, cytoplasmic, apical, and apical/cytoplasmic. It appears fairly specific for prostate, although Mhawech-Fauceglia, et al. found 17% of urothelial carcinomas to have cytoplasmic expression. In non-prostate normal tissues, PSMA showed weak cytoplasmic expression in endometrial glands, testis, bladder, and kidney tubules. Moderate cytoplasmic expression was seen in pancreas islets, GI tract ganglion cells, and brain, and strong cytoplasmic expression was seen in heart tissue.
Mhawech-Fauceglia, et al. only showed 66% sensitivity for PSMA, but this study was performed on 6 mm core punch tissue-microarray (TMA) using the YPSMA-1 clone (1:50, GeneTex, Inc., San Antonio, TX). Mohanty, et. al. showed 100% sensitivity for PSMA in a study of poorly differentiated prostate andenocarcinomas of the bladder neck using the 1D6 clone (1:20, Novocastra, Leica, Buffalo Grove, IL). It is unclear if the difference between the studies is the clone used, or that Mhawpch-Fauceglia, et al. used a small TMA, while Mohanty, et. al. used whole sections. Additional study is required in this area, and it is advisable if one chooses to use this antibody (or bring it into their lab), one should verify the performance in-house.
The specificity of PSMA is a bit difficult to completely characterize. Mhawpch-Fauceglia, et al. studied 987 benign tissues and 2,174 malignant tumors. A small subset (usually 15% or less) of a wide variety of tumors showed some expression (usually weak). Please refer to the references for a complete description beyond this brief summary. Expanded data on the 1D6 clone, similar to the Mhawpch-Fauceglia et al. paper on the YPSMA-1 clone, is not available to our knowledge.
Study
Prostate
Adenocarcinoma
Urothelial
Carcinoma
Mhawech-Fauceglia, et. al.
(YPSMA-1, 1:50, GeneTex)
66% + (N=141)
17% + (N=346)
Mohanty, et. al.
(1D6, 1:20, Novocastra)
100% + (N=20)
0% + (N=16)
References:
Mohanty SK, Smith SC, Chang E, et al. Evaluation of contemporary prostate and urothelial lineage biomarkers in a consecutive cohort of poorly differentiated bladder neck carcinomas. Am J Clin Pathol. 2014;142(2):173–183. doi:10.1309/AJCPK1OV6IMNPFGL.
Mhawech-Fauceglia P, Zhang S, Terracciano L, et al. Prostate-specific membrane antigen (PSMA) protein expression in normal and neoplastic tissues and its sensitivity and specificity in prostate adenocarcinoma: an immunohistochemical study using mutiple tumour tissue microarray technique. Histopathology. 2007;50(4):472–483. doi:10.1111/j.1365-2559.2007.02635.x.
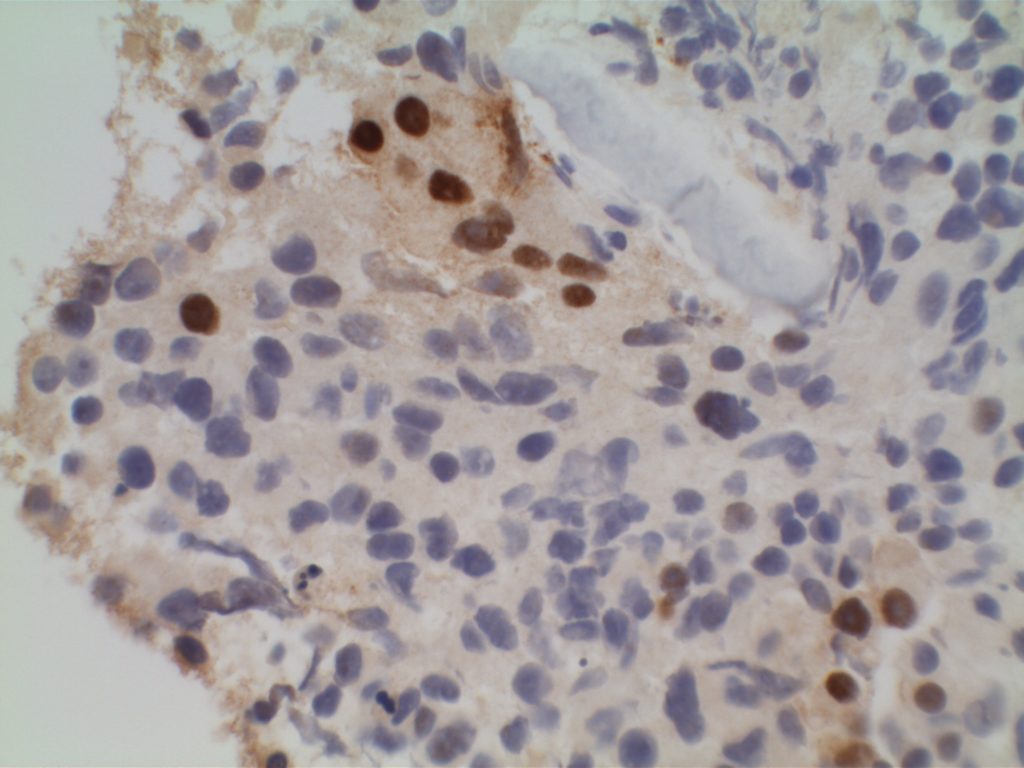
Progesterone receptor (PR) is used along with ER as a prognostication marker in breast carcinoma. Expression is determined by percent positive and intensity (1+, 2+, 3+). PR is not as important of a prognostic marker compared to ER, but lower grade more differentiated tumors tend to show stronger expression of both ER and PR, and also have a better relative treatment outcome compared higher grade tumors.
A PR positive, ER negative, expression pattern should raise concern that either the slides were mislabeled, or the ER assay may not be performing properly. Most believe that ER expression is required for PR expression.
Outside of being used as a breast predictive marker, PR is not used too much in routine diagnostic surgical pathology.
Summary
Nuclear Marker
Stain is reported as PERCENT STAINING OF TUMOR CELLS and STAIN INTENSITY (1+, 2+, 3+)
1% or greater nuclear expression in tumor cells is considered positive
PR expression is a prognostic marker, and not directly used for eligibility to receive a specific treatment
PR expression without ER expression should raise significant concern that the ER and PR slides have been mixed up, or there is a problem with the ER assay. Many scientists believe that ER expression is required for PR expression.
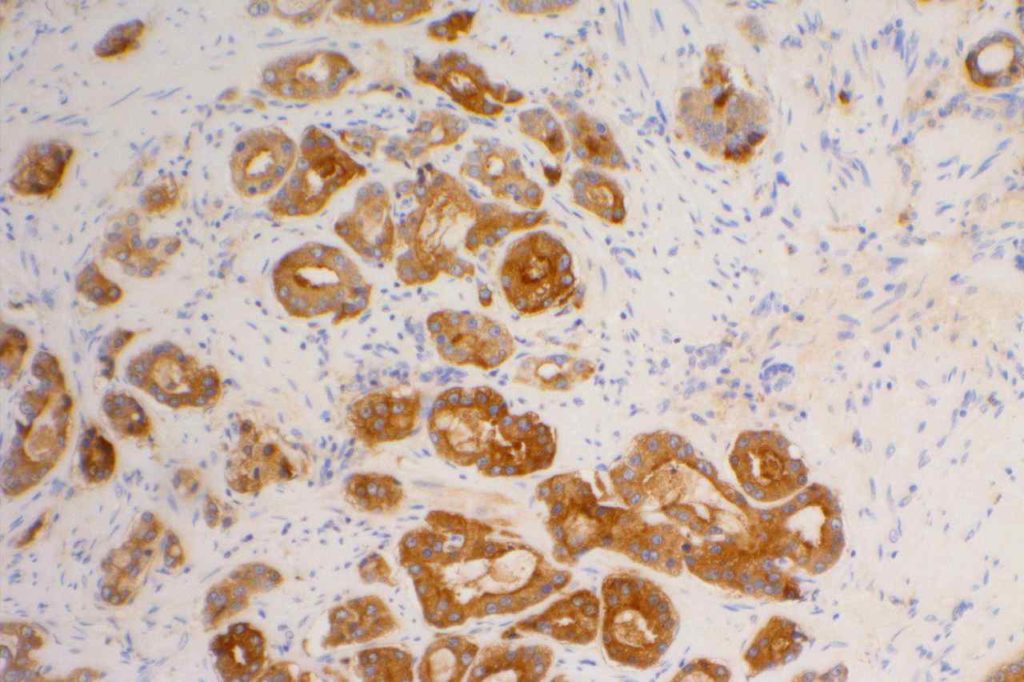
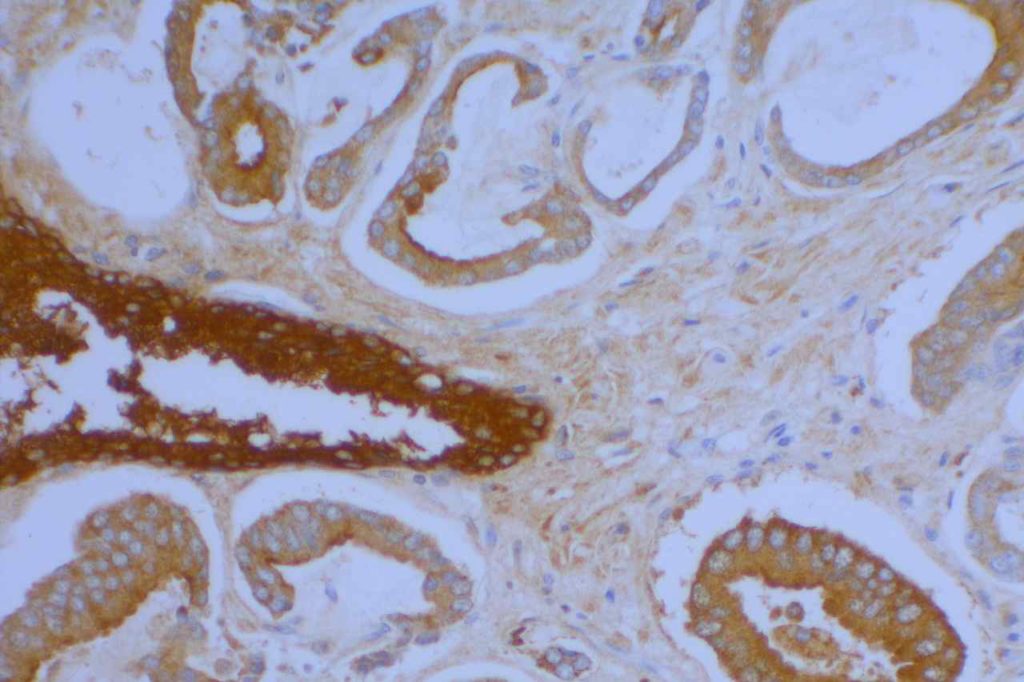
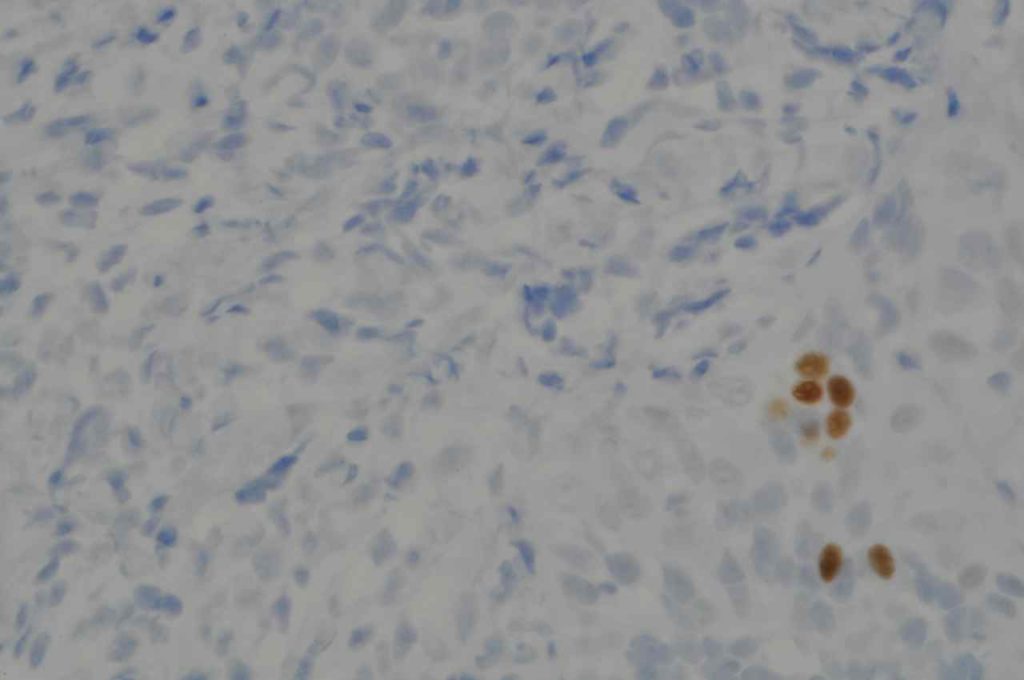
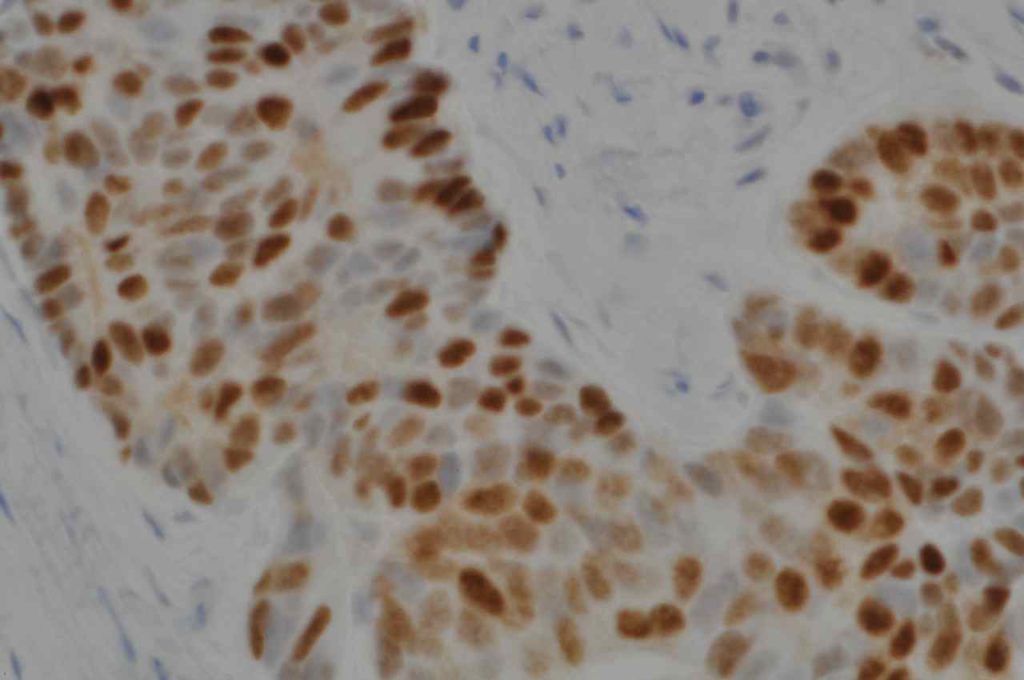
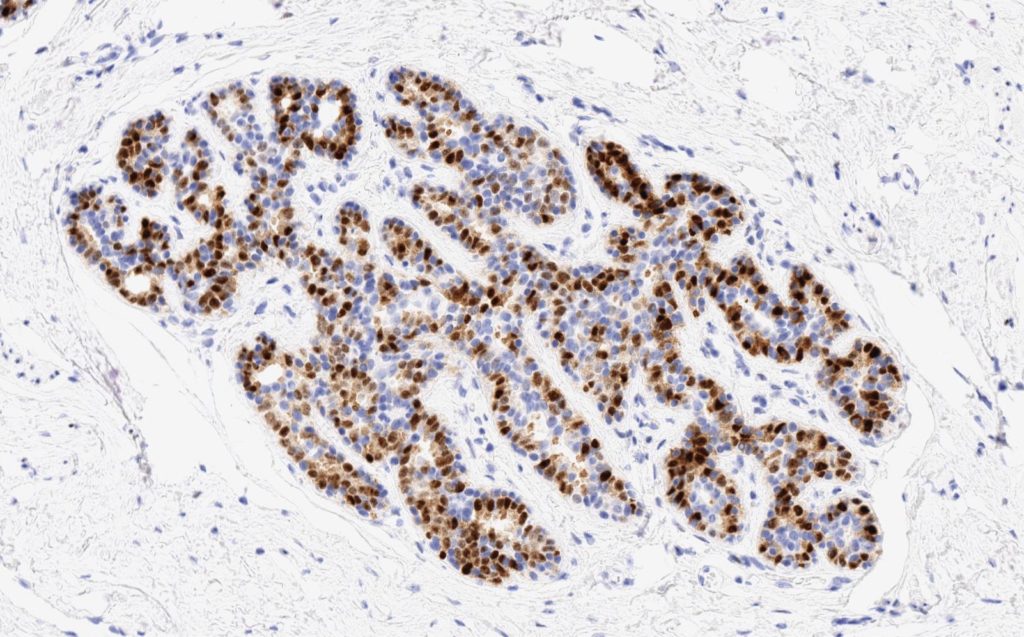
Photomicrographs
PR – Metastatic Breast Carcinoma (focal expression)PR – Breast Carcinoma (moderate to strong expression)PR – Normal Breast
References
Hammond ME, et. al. “ASCO-CAP Guideline Recommendations for IHC Testing of ER and PR in Breast Cancer”. Arch Pathol Lab Med-Vol. 134, June 2010.