Lysozyme (LZ) is similar to myeloperoxidase (MPO) in that they are associated with cytoplasmic bactericidal granules, which are specific for myeloid differentiation. LZ is most useful along with other markers such as MPO and CD117 in identifying case of AML, in which none of the markers are entirely sensitive.
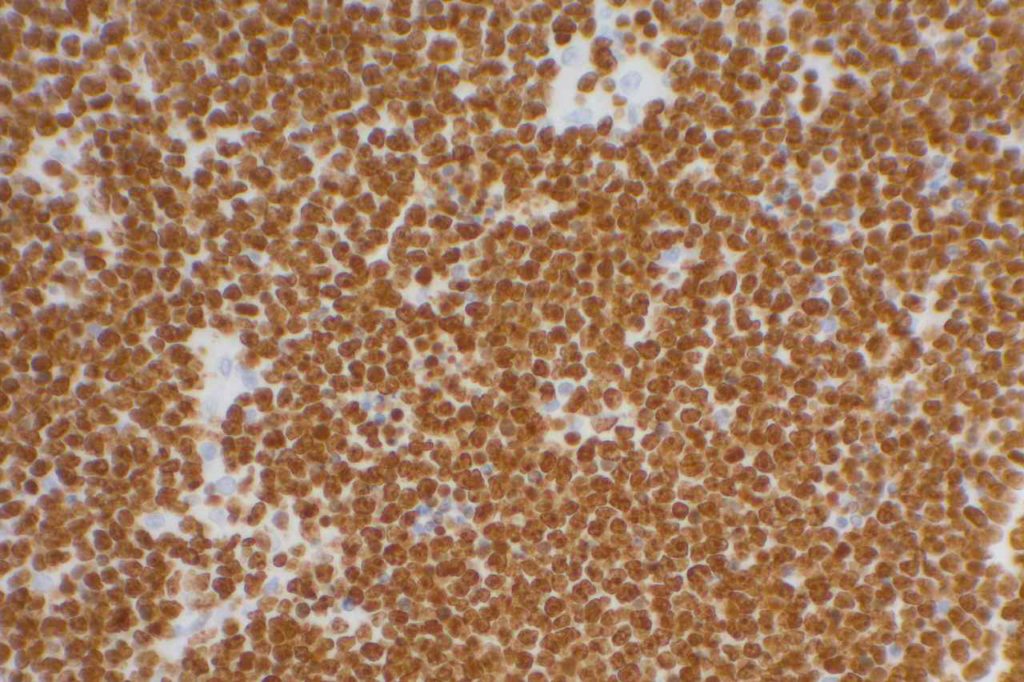
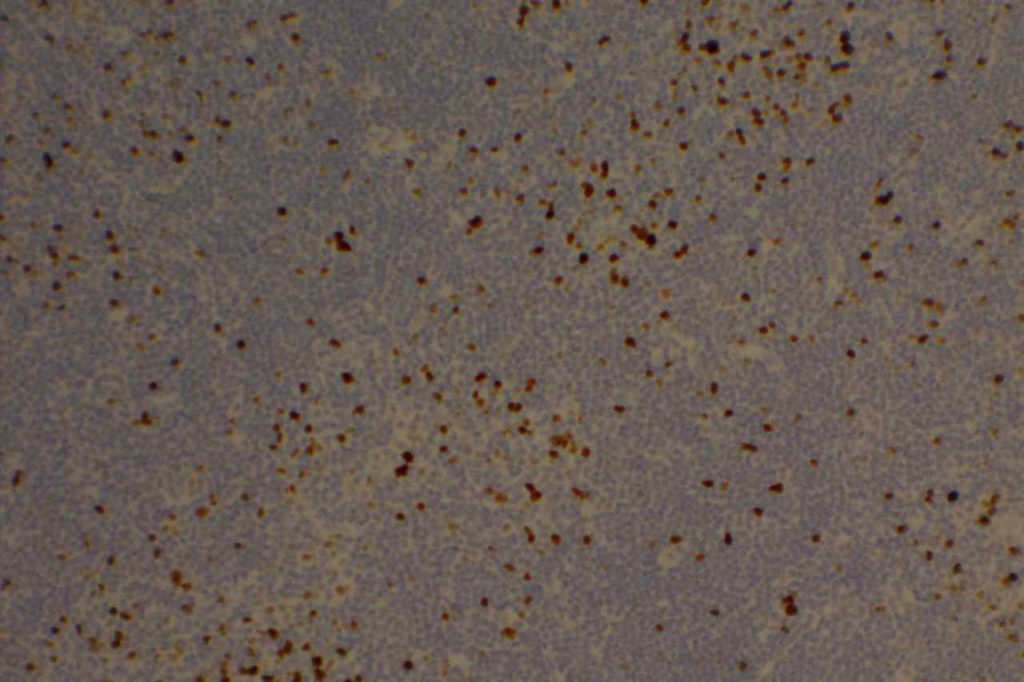
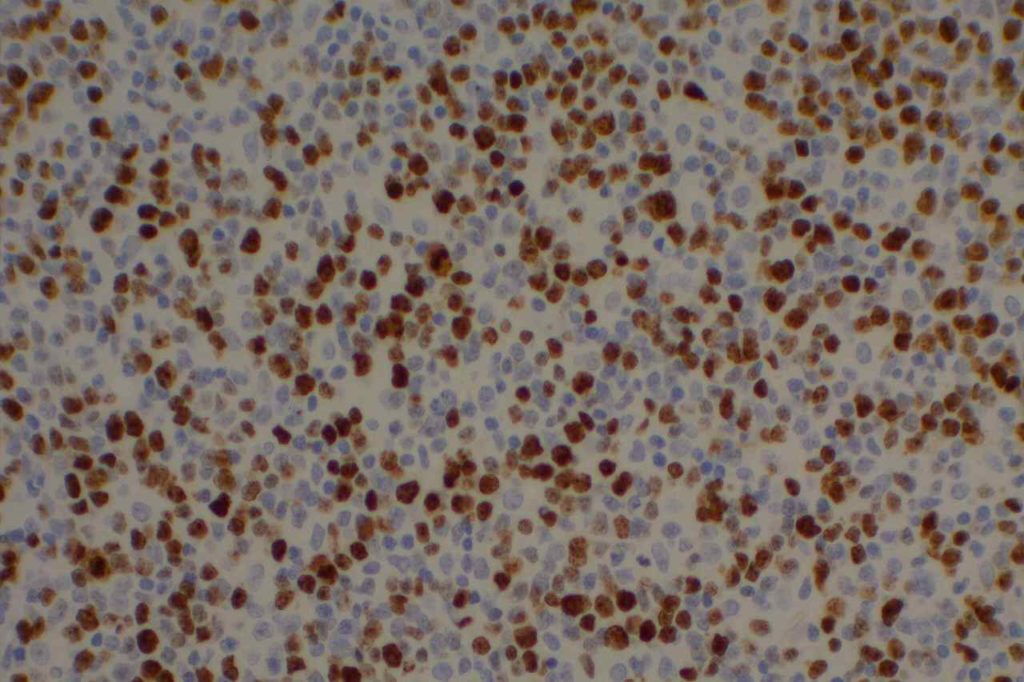
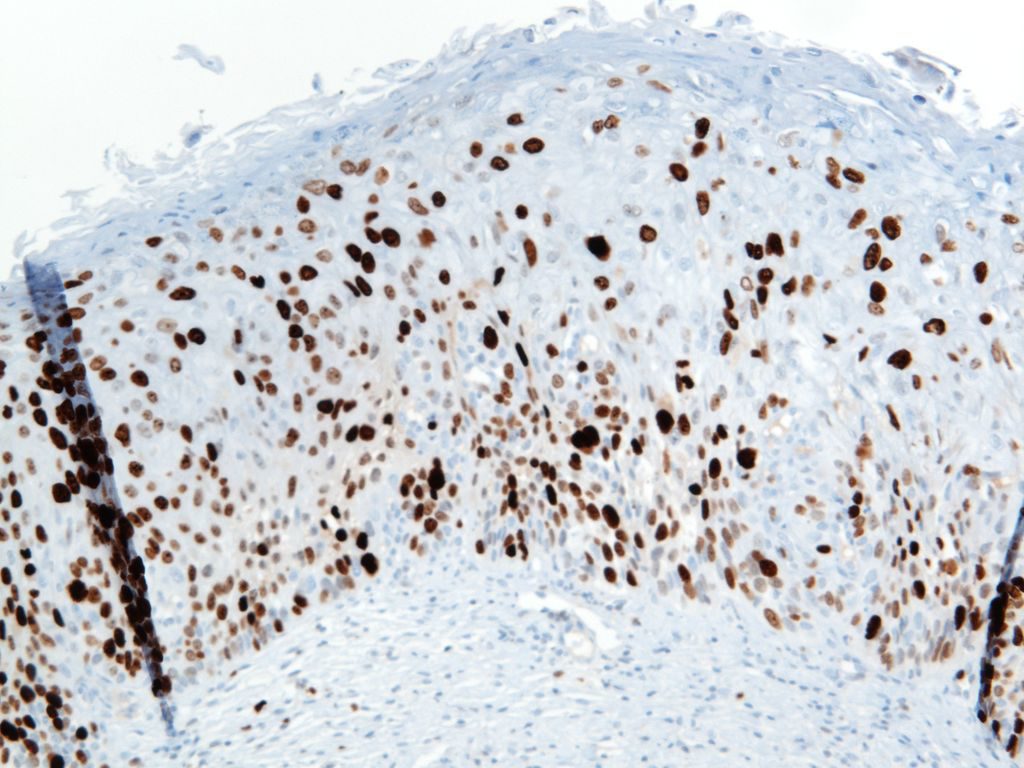
Ki-67 is a proliferation marker with nuclear staining. It is expressed in cells in G1, S, G2 and M phases of the cell cycle. This marker is used in many ways, and often carries prognostic information for many malignancies (breast, certain lymphomas, etc.). It is also used as a diagnostic aid in certain difficult cases (e.g. cervical dysplasia, melanocytic tumors, etc.).
When using this stain diagnostically, one should understand the clinical significance for the diagnostic circumstance in which the stain is being used, and have appropriate knowledge of the medical literature with respect to the staining performance in the given clinical-pathologic setting. For example low grade lymphomas would be expected to have a relatively low-proliferation staining index (<30%), whereas Burkitt Lymphoma would have a high staining index (>95%).
Katzenberger, T., Petzoldt, C., Höller, S., Mäder, U., Kalla, J., Adam, P., et al. (2006). The Ki67 proliferation index is a quantitative indicator of clinical risk in mantle cell lymphoma. Blood, 107(8), 3407. doi:10.1182/blood-2005-10-4079
McCall, C. M., Shi, C., Cornish, T. C., Klimstra, D. S., Tang, L. H., Basturk, O., et al. (2013). Grading of well-differentiated pancreatic neuroendocrine tumors is improved by the inclusion of both Ki67 proliferative index and mitotic rate. The American Journal of Surgical Pathology, 37(11), 1671–1677. doi:10.1097/PAS.0000000000000089
Kappa/Lambda (K/L) may be performed by immunohistochemistry (IHC) or in situ hybridization (ISH). K/L studies is primary used in the evaluation of plasma cell disorders or lymphoproliferative disorders containing some level of plasmacytoid differentiation. In tissue sections IHC for K/L often produces a large amount of background staining, which makes its use more difficult on a day-to-day basis compared to ISH (much less background).
The second big issue in K/L staining is that it is often performed on decalcified bone marrow biopsy core sections. The decalcification process may cause significant issues in the sensitivity of both IHC and ISH. As an alternative, always making a clot section on bone marrow specimens may greatly increase diagnostic yield and reliability.
Determination of monoclonality of plasma cells can sometimes be challenging. Historically, most consider a K:L ratio <0.5 or >4.0 to be indicative of monoclonality. Like almost everything in pathology, holding to a specific and tight threshold may put one in a perilous position in making a diagnosis. By flow cytometry, Samoszuk, et. al found that K:L ratios <0.7 and >5.5 were optimum for discriminating between lymphoma and benign hyperplasia (false negative rate= 27%, and false positive rate= 6%).
Evaluating K:L ratios in tissue sections is generally analogous to flow cytometry. Normally, there are 2-4 Kappa plasma cells to every Lamdda plasma cell. A ratio of K:L > 8:1 or a L:K ratio > 4:1 is strongly suggestive of a monoclonal plasma cell population.
Practically, if K:L ratio is no “obviously” monoclonal on ISH/IHC, it may be best to identify it as a kappa or lambda predominate population and correlate with other laboratory, radiologic and clinical findings. A significant pitfall may occur when either the kappa or lambda stain doesn’t work, and the case looks like a monoclonal population. Even in “obvious” monoclonal cases, one should be able to find a rare kappa or lambda staining plasma cell. If not, then the maker should be repeated.
Photomicrographs
Hematopathology – Part 4, Question #7. Kappa.Hematopathology – Part 4, Case #2. Kappa (ISH)Kappa ISH staining of plasma cells. ISH staining usually has cleaner staining with less background staining compared to conventional IHC staining.Kappa ISH staining of plasma cells. ISH staining usually has cleaner staining with less background staining compared to conventional IHC staining.
References
Parker, A., et. al. “Best Practice in Lymphoma Diagnosis and Reporting.” British Committee for Standards in Haematology, Royal College of Pathologists. April, 2010.
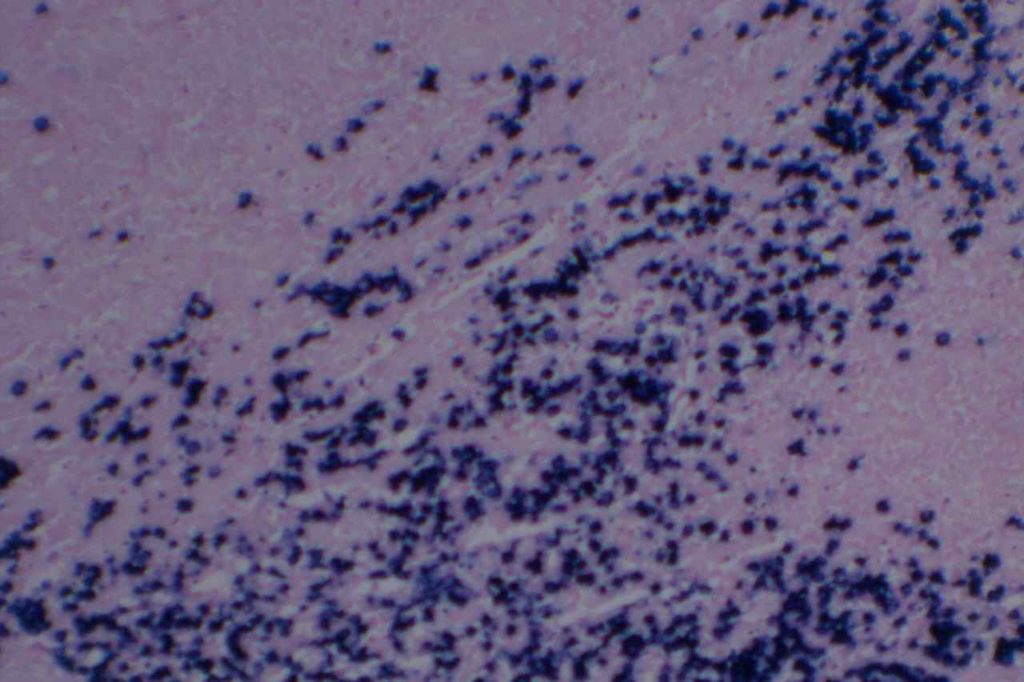
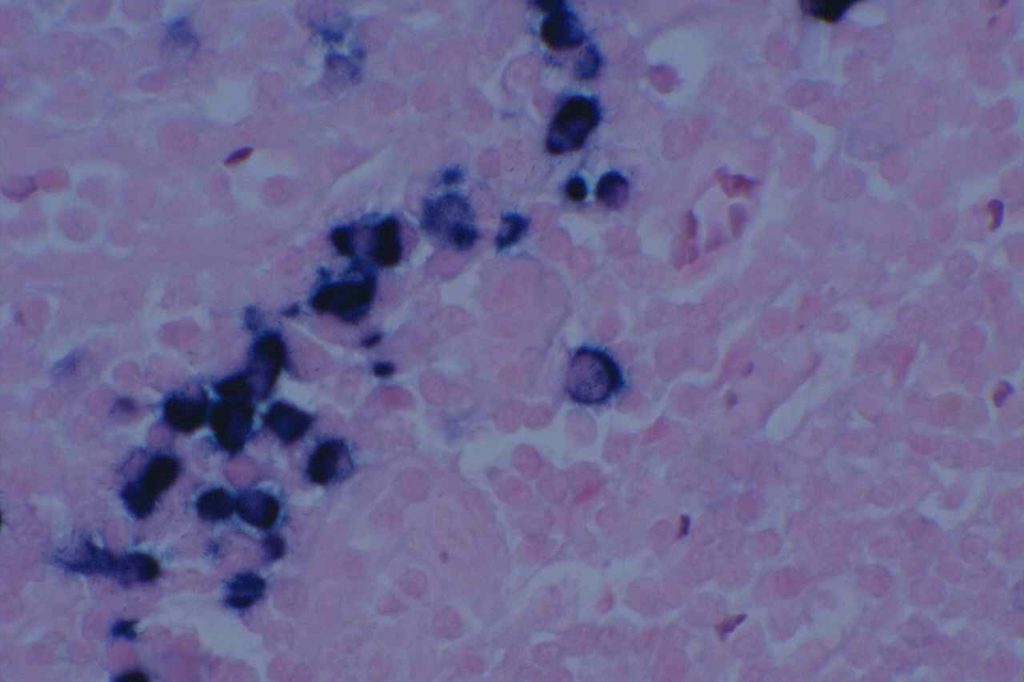
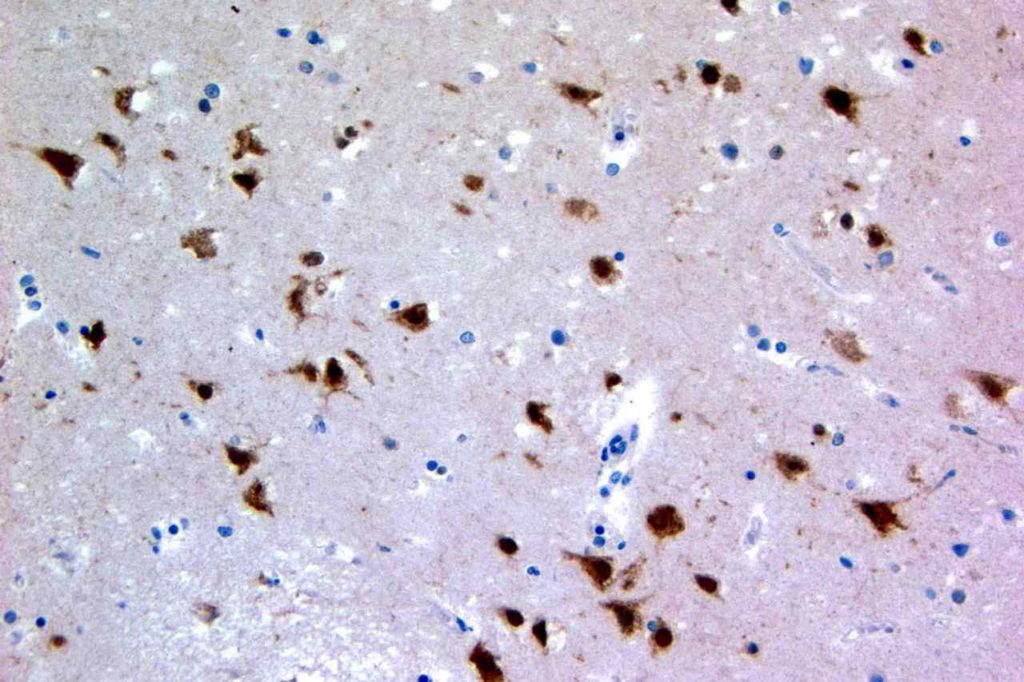
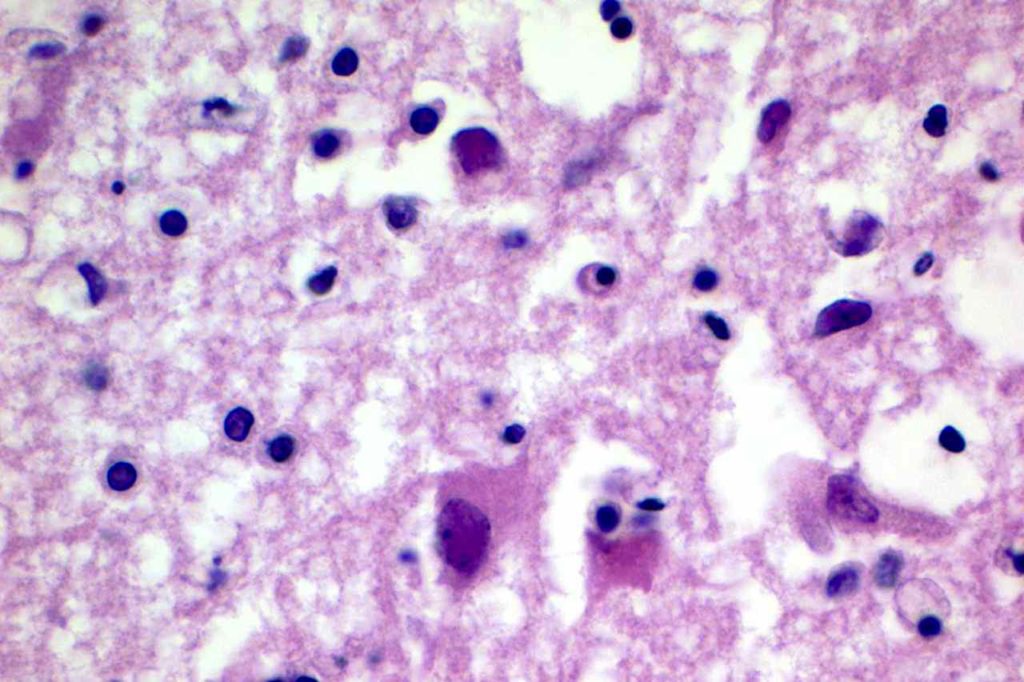
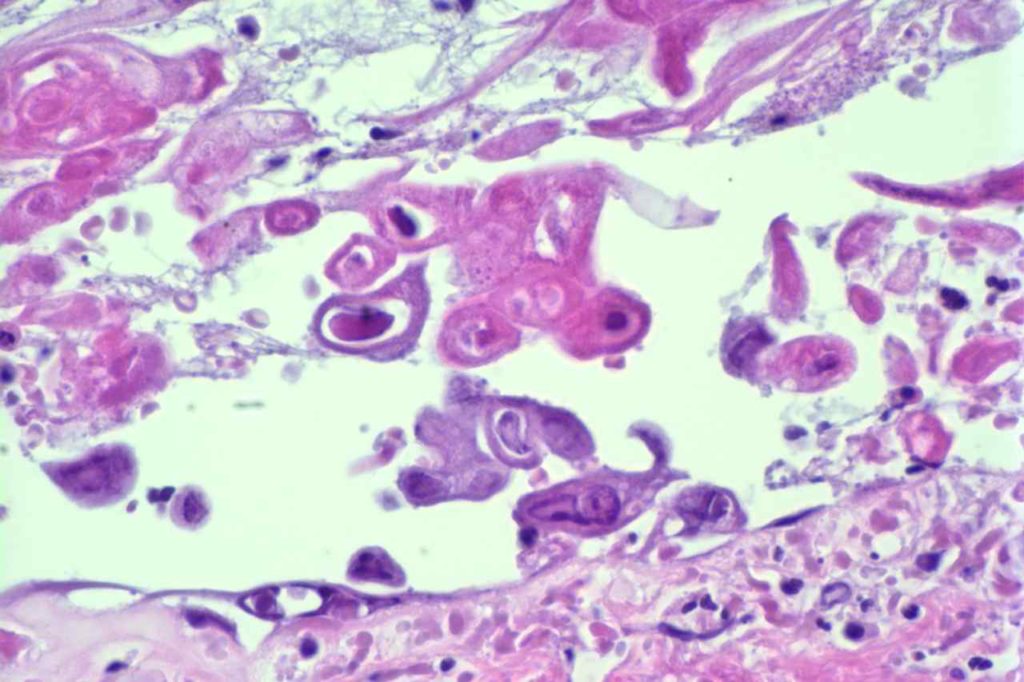
Herpes Simplex Virus (HSV) is a virus, which causes a painful skin/mucosal blistering disorder that can involve numbers areas including genitalia, lips, esophagus, and skin. Immunohistochemistry (IHC) antibodies for HSV-1 and HSV-2 are available for testing in paraffin embedded tissue. In general, HSV-1 infections are more common above the diaphragm, and HSV-2 are more common below the diagram. While the availability of HSV-1 specific and HSV-2 specific antibodies for testing might suggest they are highly specific. In the author’s experience, there is a lot of cross reactivity between the HSV-1 and HSV-2 antibodies, and one should not consider positivity as definitively specific.
Photomicrographs
HSV IHC staining in brain with HSV infection.HSV infection of the brain.H&E – HSV esophagitisHSV Esophagitis
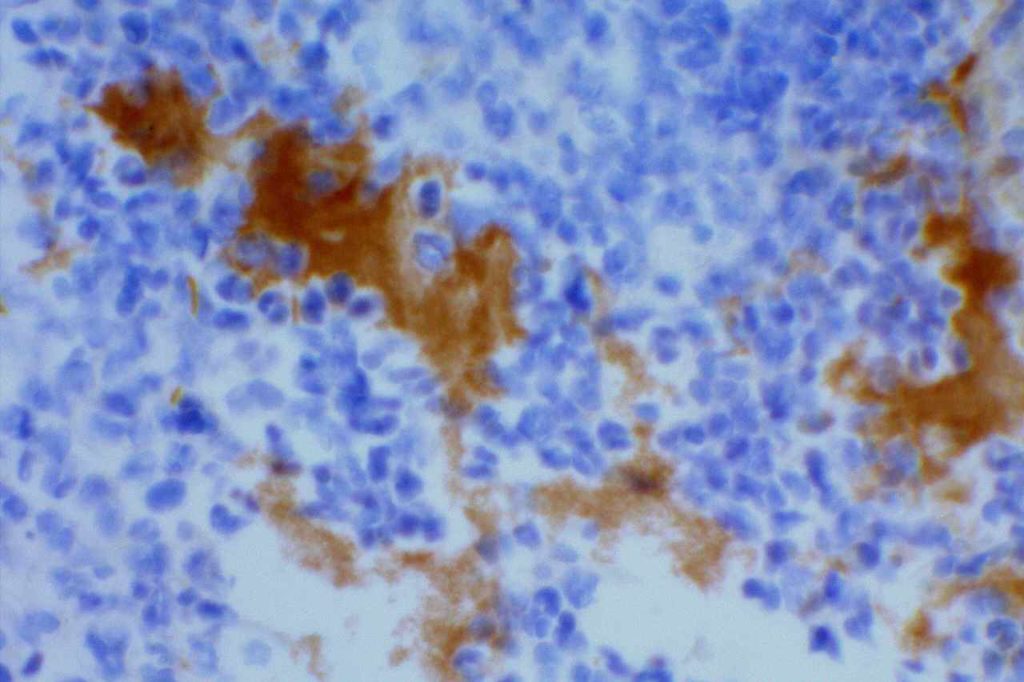
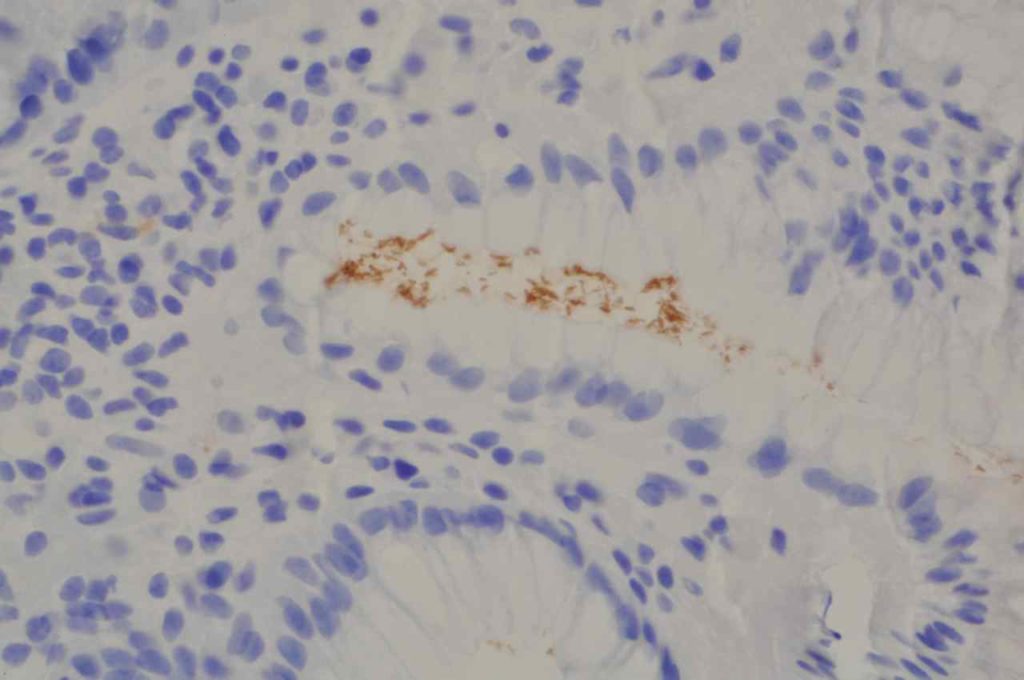
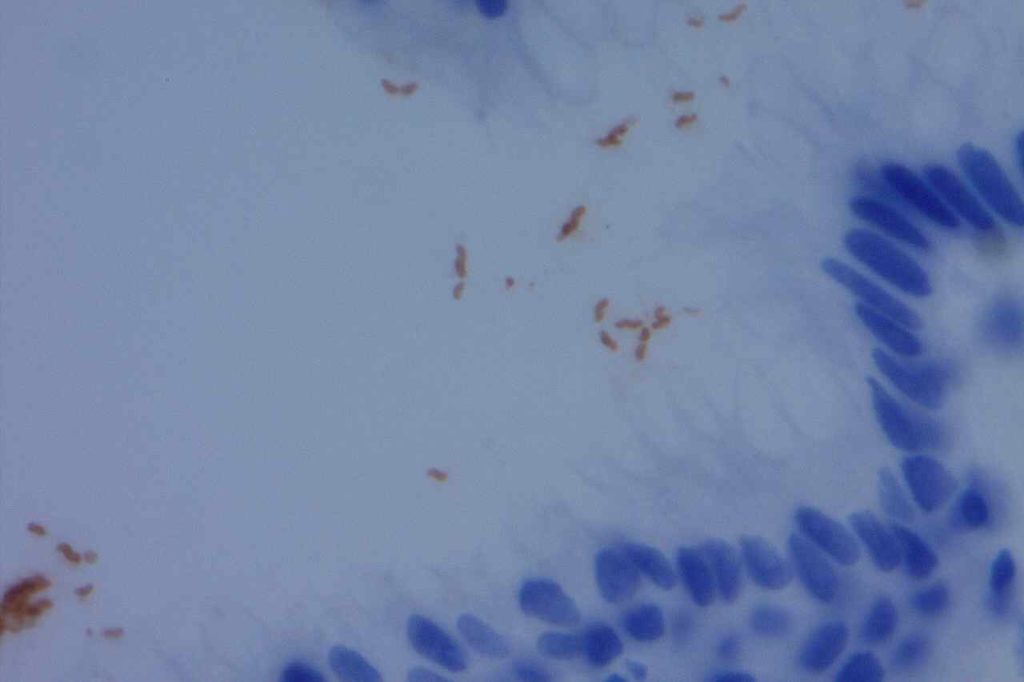
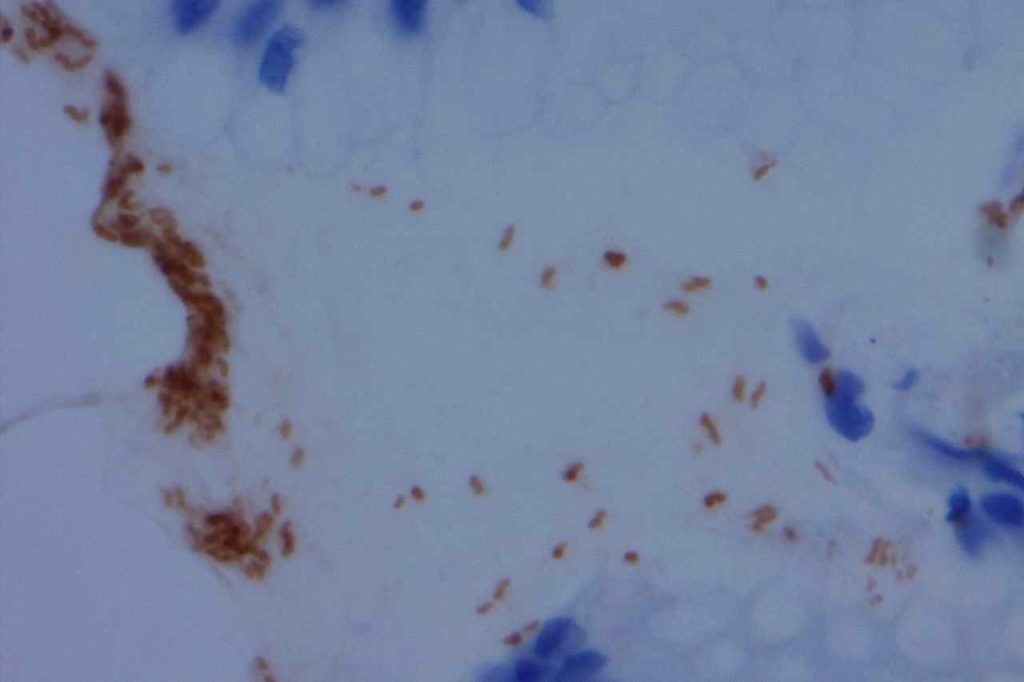
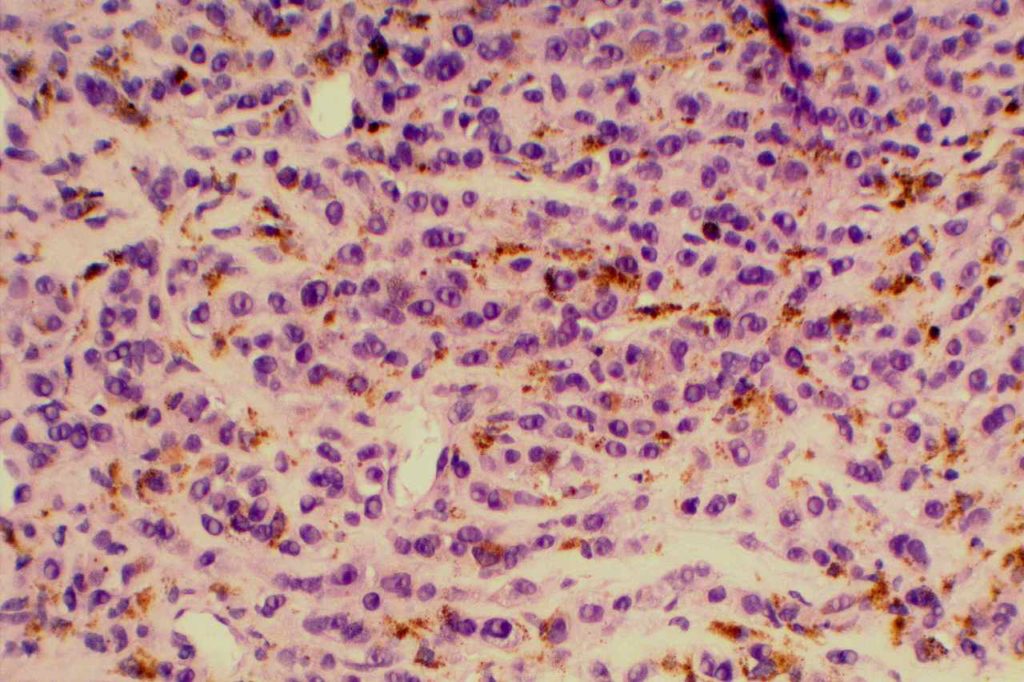
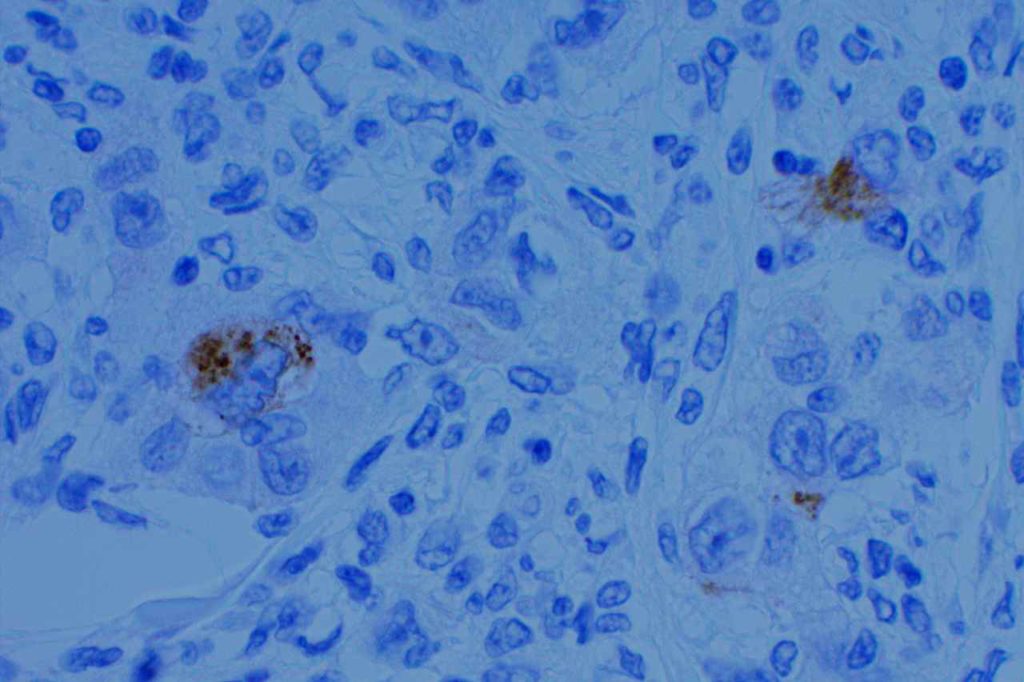
Monoclonal and polyclonal antibodies are available to H. pylori for use in paraffin embedded tissue. While less specific, other stains (e.g. silver stains, Giemsa, modified Steiner, etc.) may be used to highlight the bacterial organisms. IHC stains provide the most sensitive and specific marker for identification. Additionally, IHC stains for H. pylori have much lower background than special stains, making it easier for the pathologist to make the diagnosis.
Stain Interpretation
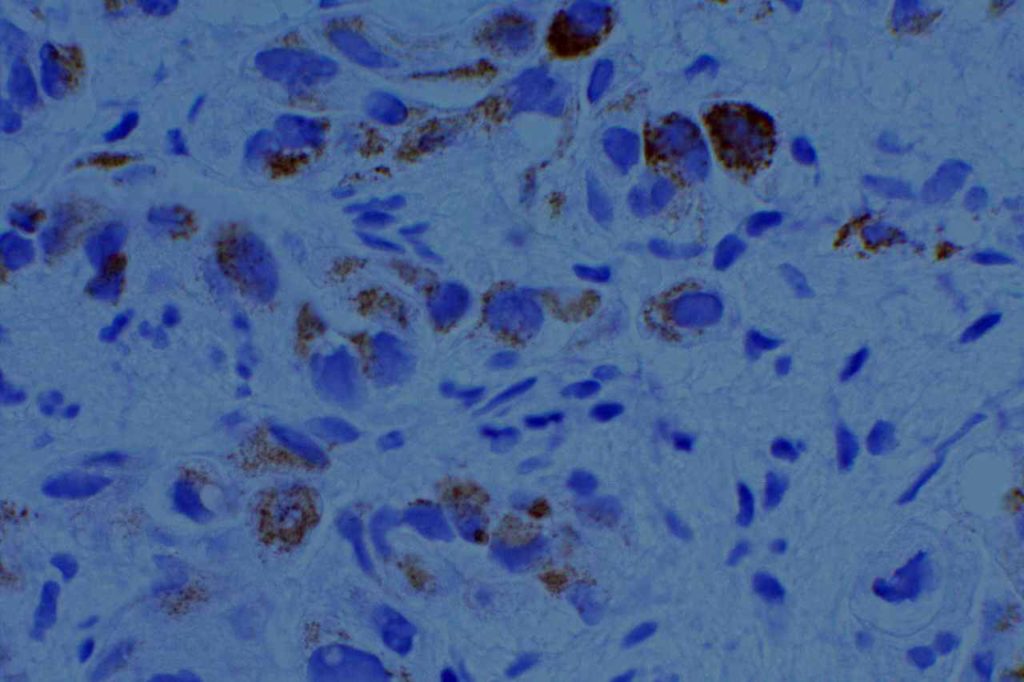
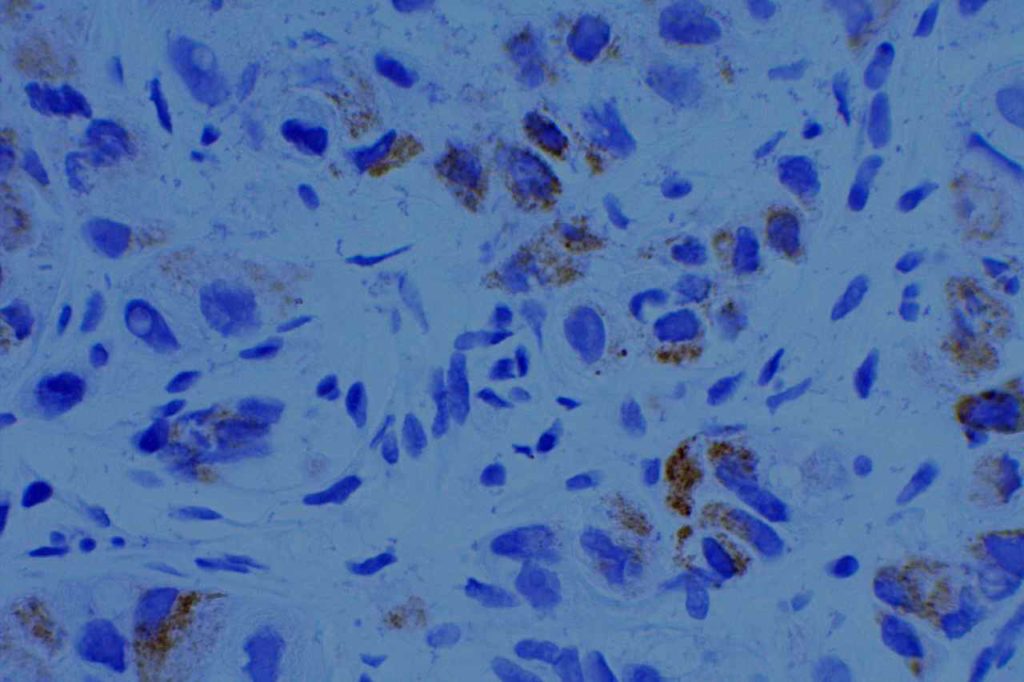
For a case to be positive, there must be staining and bacterial morphology (curvilinear organisms). There are several pitfalls to be aware of to interpret H. pylori stains:
“Junk Staining” on the surface as a result of neutral red or other pigmented stains used as the time of grossing to help visualize tissue while cutting. This most commonly occurs when stains used at the grossing station are not filtered regularly (or are just old) with subsequent precipitate material.
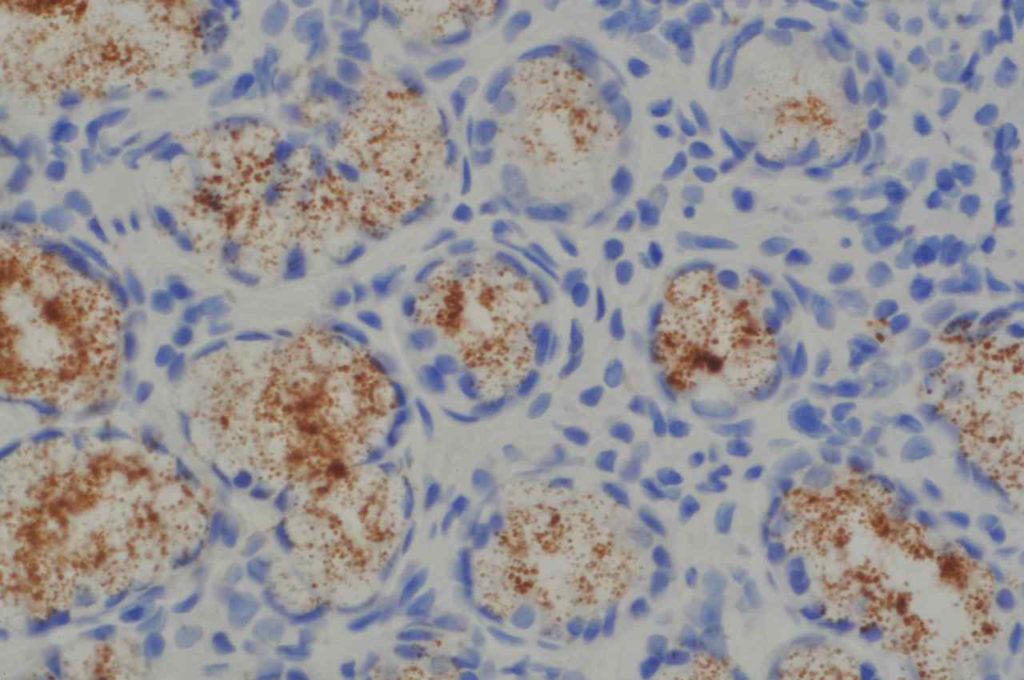
Some antibodies (e.g. Novocastra monoclonal) may show cross-reactivity with cytoplasmic antral gland granules. This is most confusing when the granules are dislodged from the cytoplasmic location during the biopsy procedure and are distributed along the mucosal surface. They have a characteristic appearance of variably sized round granules.
Stain Sensitivity and Specificity (Hartman, et al)
Stain
Sensitivity
Specificity
H&E
83%
100%
Giemsa
62%
97%
Warthin-Starry
62%
98%
IHC Staining
97-100%
100%
General Comment
The Rodger C. Haggitt Gastrointestinal Pathology Society has published a consensus recommendation that special stains to evaluate for Helicobacter organisms are appropriate when there is chronic gastritis or chronic active gastritis without evidence of organisms on routine H&E sections. Routine performance of special stains upfront on all biopsies for Helicobacter is NOT recommended. (Batts, et al)
Please see the image example for demonstration of proper staining and artifacts.
H. pylori IHC stain highlighting Helicobacter organisms.H. pylori IHC stain highlighting Helicobacter organisms.H. pylori IHC stain highlighting Helicobacter organisms.H. pylori (monoclonal) IHC stain highlighting granules in antral glands. This should not be misinterpreted as positive for H. pylori organisms. Round granules from these glands can be displaced during biopsy procedure, which can be located on the mucosal surface causing further confusion.
References:
Hartman, D. J., & Owens, S. R. (2012). Are routine ancillary stains required to diagnose helicobacter infection in gastric biopsy specimens?: an institutional quality assurance review. American Journal of Clinical Pathology, 137(2), 255–260. doi:10.1309/AJCPD8FFBJ5LSLTE
Riba, A. K., Ingeneri, T. J., & Strand, C. L. (2011). Improved Histologic Identification of Helicobacter pylori by Immunohistochemistry Using a New Novocastra Monoclonal Antibody. Laboratory Medicine, 42(1), 35–39. doi:10.1309/LMAGPAENJKNARI4Z
Batts, K. P., Ketover, S., Kakar, S., Krasinskas, A. M., Mitchell, K. A., Wilcox, R., et al. (2013). Appropriate use of special stains for identifying Helicobacter pylori: Recommendations from the Rodger C. Haggitt Gastrointestinal Pathology Society. The American Journal of Surgical Pathology, 37(11), e12–22. doi:10.1097/PAS.0000000000000097
HMB-45 (Human Melanoma Black) is a monoclonal antibody to melanosomal glycoprotein gp100, and is relatively specific for melanocytes. The staining pattern is cytoplasmic. Similar to MART1, HMB-45 is less sensitive for melanoma when it has a spindle cell pattern. S-100 (less specific) is a better screening marker than HMB-45 or MART1. HMB-45 is better as a confirmatory marker.
HMB45 will stain: angiomyolipoma, melanoma, soft part sarcoma, sugar tumor of lung, lymphangiomyomatosis, pheochromocytoma (30%), pigmented nerve sheath tumors, and benign nevi / melanocytes. It is also important to understand that some histiocytes in lymph nodes may stain with HMB-45, which must be differentiated from metastatic melanoma cells. At least some histiocytes stained with HMB-45 in 50% of lymph nodes in a study by Hutchens, KA, et al.
HMB-45 will mark melanocytes and melanocytic derived neoplasms, but is not diagnostic in and of itself of anything abnormal. Dysplasia/neoplasia can only be diagnosed on the H&E slide after confirming morphology and/or melanocytic cell distribution with IHC analysis.
Photomicrograph
HMB-45 expression in melanoma. Red chromogen if helpful in distinguishing tumor cells from non-tumor pigmented cells.HMB-45 expression in melanoma.
Reference
Hutchens, K. A., Heyna, R., Mudaliar, K., & Wojcik, E. (2013). The new AJCC guidelines in practice: utility of the MITF immunohistochemical stain in the evaluation of single-cell metastasis in melanoma sentinel lymph nodes. The American Journal of Surgical Pathology, 37(6), 933–937. doi:10.1097/PAS.0b013e3182815574
Kucher, C., Zhang, P. J., Acs, G., Roberts, S., & Xu, X. (2006). Can Melan-A replace S-100 and HMB-45 in the evaluation of sentinel lymph nodes from patients with malignant melanoma? Applied Immunohistochemistry & Molecular Morphology : AIMM / Official Publication of the Society for Applied Immunohistochemistry, 14(3), 324–327.
HER2 (Human Epidermal growth Factor Receptor 2), which is also known as c-erb2, net, ERBB2, and CD340 is a member of the human epidermal growth factor receptor family (HER1, HER2, HER3, and HER4). Interestingly HER1 is also known as EGFR (epidermal growth factor receptor).
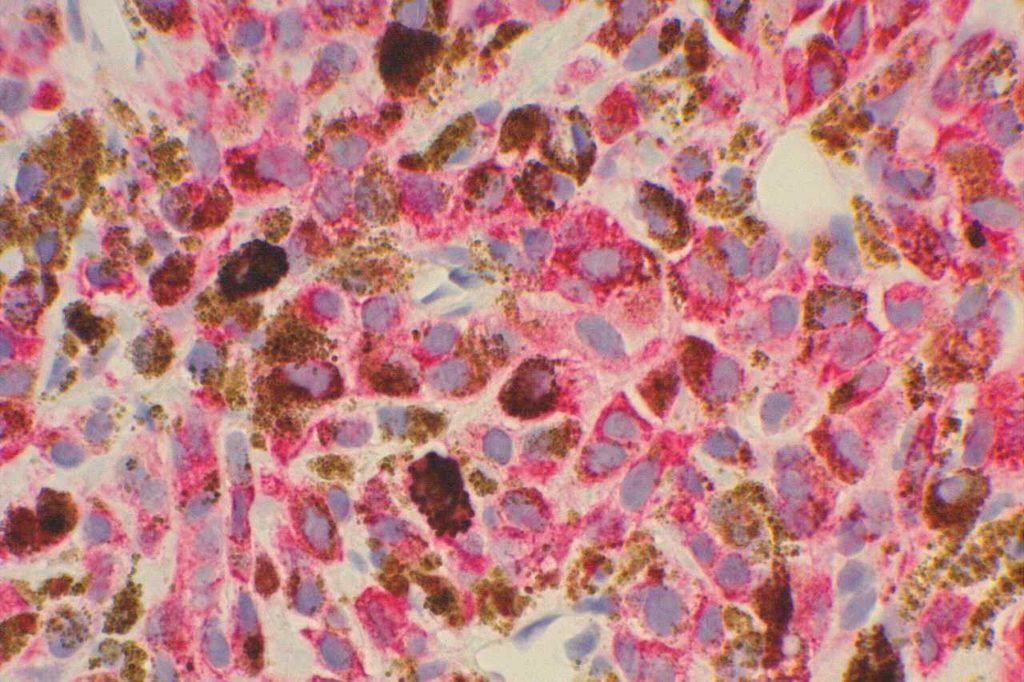
HepPar-1 is a mitochondrial antigen present in normal hepatocytes, and is a relatively specific marker for hepatic origin. It also stains approximately 80-100% of hepatocellular carcinomas. It is most commonly used to help identify tumors of primary hepatic origin, and exclude cholangiocarcinoma in the differential diagnosis.
Interpretation
The staining pattern is granular and cytoplasmic in location. The staining pattern can be heterogeneous ranging from focal (<5%) in poorly differentiated HCC to strong diffuse staining in well-differentiated HCC. As with most issues in pathology and IHC, less differentiated lesions more often need IHC, which tend to perform less-optimally than described in the literature (case selection bias). Also beware of focal staining of benign entrapped hepatocytes.
Specificity
HepPar-1 is not a pertfectly specific marker for HCC. One study (Wee) notes specificity as 73% with non-hepatic tumors including adenocarcinomas from lung, gallbladder, pancreas, stomach, small intestine, adenoma of colon, adrenal gland carcinoma, paraganglioma, and melanoma showing expression. Other studies show the specificity near 90% for HCC.
Up to 25% (probably <10% overall) of lung carcinomas (mostly adenocarcinomas) have been noted to have HepPar1 expression (cytoplasmic and granular). The expression pattern may be focal/patchy, but these tumors also typically express TTF-1.
Use of HepPar-1 as part of a panel (and clinical-radiologic correlation) is recommended for optimal interpretation.
Wee, A. (2006). Diagnostic utility of immunohistochemistry in hepatocellular carcinoma, its variants and their mimics. Applied Immunohistochemistry & Molecular Morphology : AIMM / Official Publication of the Society for Applied Immunohistochemistry, 14(3), 266–272.
Allende, D., & Yerian, L. (2009). Immunohistochemical Markers in the Diagnosis of Hepatocellular Carcinoma. Pathology Case Reviews, 14(1), 40–46.
Yousem, S. A., Lale, S., & Dacic, S. (2013). HepPar-1 expression in primary lung adenocarcinoma. American Journal of Clinical Pathology, 140(2), 225–230. doi:10.1309/AJCP4MXTNQRVOE2T
Minervi el al., 1997.
Chu et al., Am J Surg Pathol 26:978-88, 2002.
L. Lamps. “The Differential Diagnosis of Hepatic Tumors.” UAMS, Lecture, 2005.
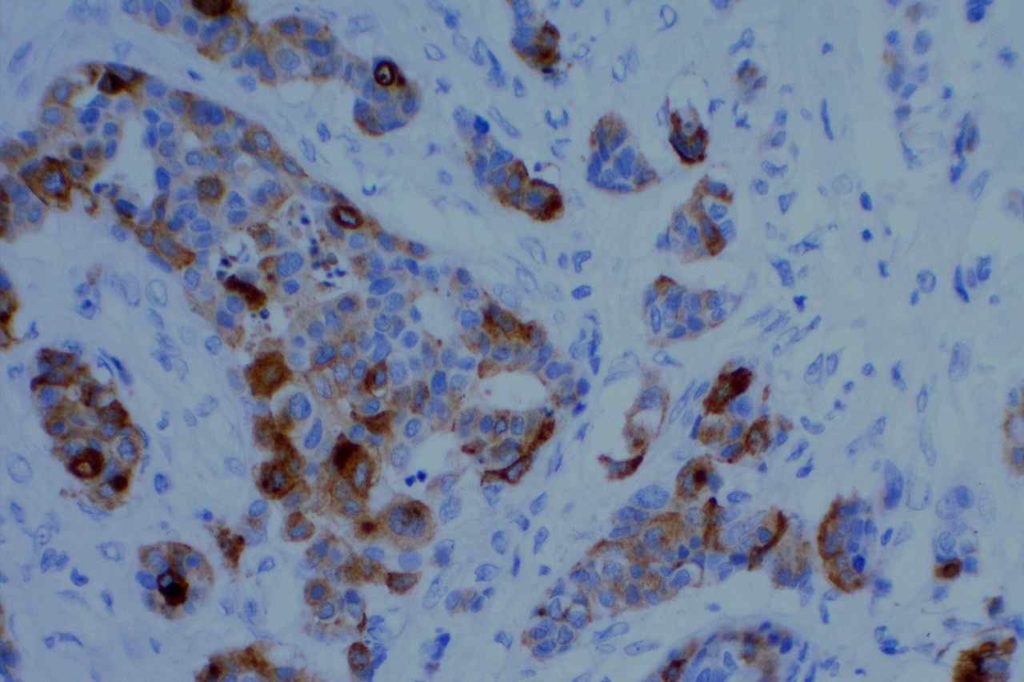
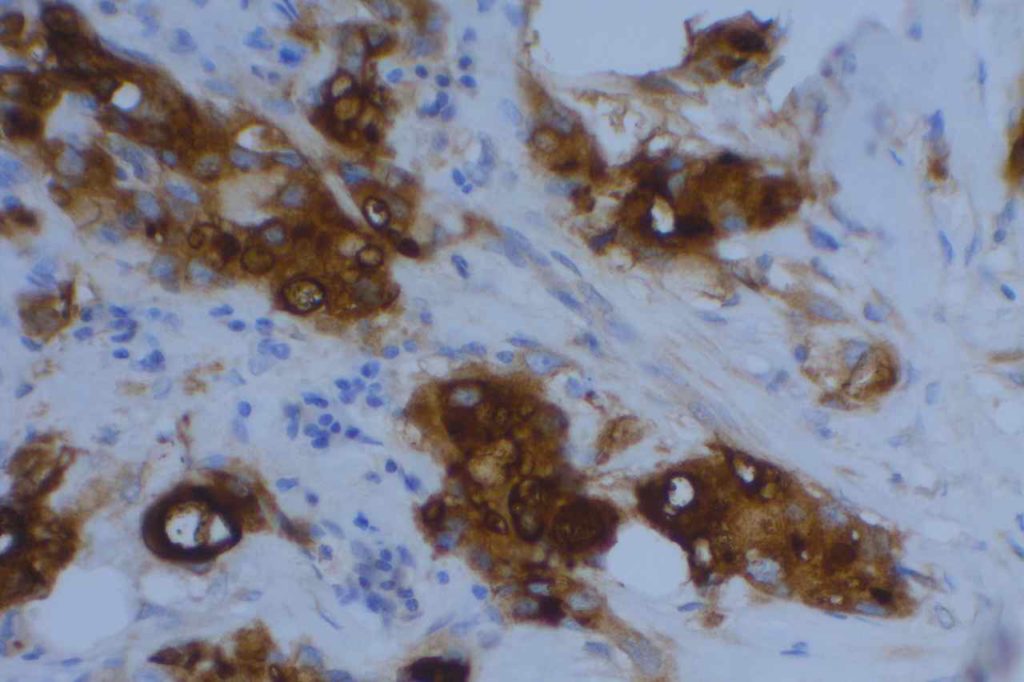
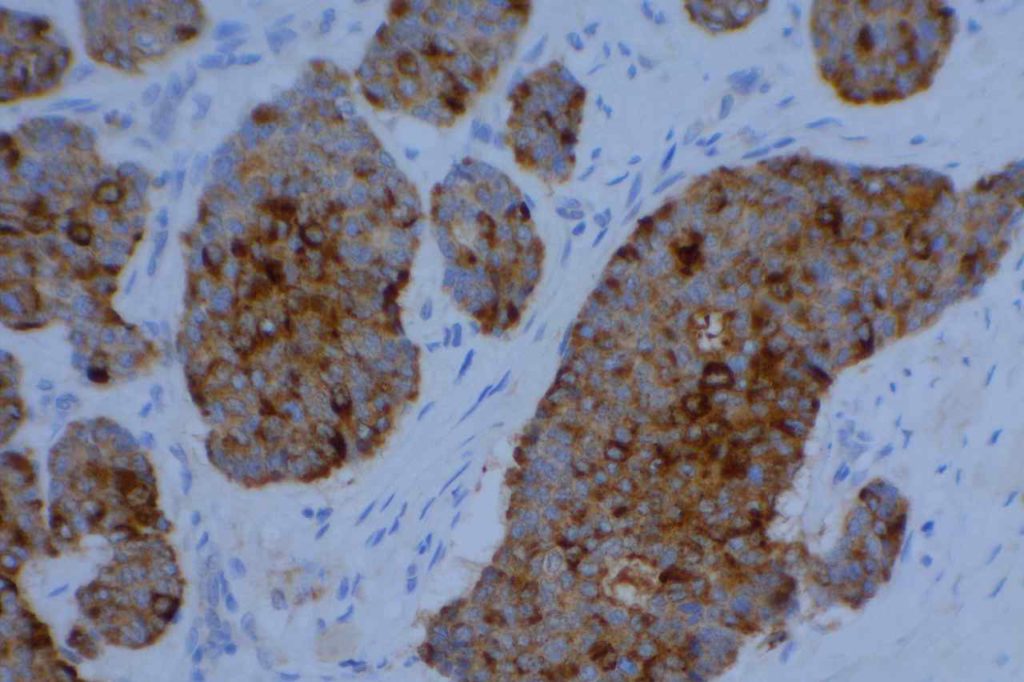
Gross Cystic Disease Fluid Protein 15 (GCDFP-15) is a marker derived from breast epithelium secretions. It is a marker of apocrine differentiation. In the setting diagnostic pathology, GCDFP-15 is very specific for breast carcinoma. Most basal-like breast carcinomas do not express GCDFP-15 or Mammaglobin. It also marks salivary and sweat gland tumors, but this rarely is in the differential diagnosis with breast carcinoma.
The sensitivity for breast carcinomas is in the range of 50-70%.
Common expression patterns in carcinoma [Dennis, et al and Striebel et al]:
Tumor
(%)
Breast
50-70%
Colon
<5%
Lung
up to 5%
Ovary
<5%
Pancreas
<5%
Stomach
<5%
Prostate
~10%
Photomicrographs
GCDFP-15 – Breast CarcinomaGCDFP-15 – Breast CarcinomaGCDFP-15 – Breast CarcinomaGCDFP-15 – Breast Carcinoma
References
Dennis, J. L., Hvidsten, T. R., Wit, E. C., Komorowski, J., Bell, A. K., Downie, I., et al. (2005). Markers of adenocarcinoma characteristic of the site of origin: development of a diagnostic algorithm. Clinical Cancer Research : an Official Journal of the American Association for Cancer Research, 11(10), 3766–3772. doi:10.1158/1078-0432.CCR-04-2236
Striebel, J. M., & Yousem, S. A. (2008). Gross Cystic Disease Fluid Protein – (GCDFP-15): Expression in Primary Lung Adenocarcinoma. The American Journal of Surgical Pathology, 00(00), 7.
Lewis, G. H., Subhawong, A. P., Nassar, H., Vang, R., Illei, P. B., Park, B. H., & Argani, P. (2011). Relationship between molecular subtype of invasive breast carcinoma and expression of gross cystic disease fluid protein 15 and mammaglobin. American Journal of Clinical Pathology, 135(4), 587–591. doi:10.1309/AJCPMFR6OA8ICHNH
Granzyme B is a cytoplasmic marker for cytotoxic T lymphocytes. It is used as a marker along with TIA-1 to prove cytotoxic differentiation. It is expressed in normal cytotoxic T cells and certain T cell neoplasms derived from cytotoxic T cells.