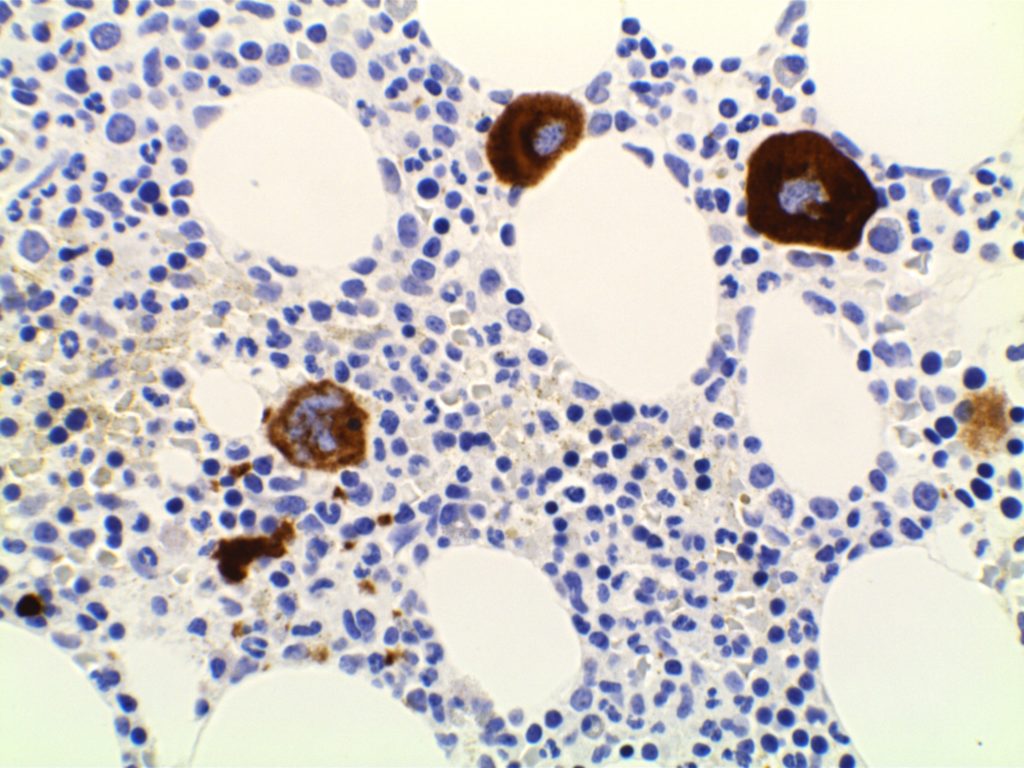
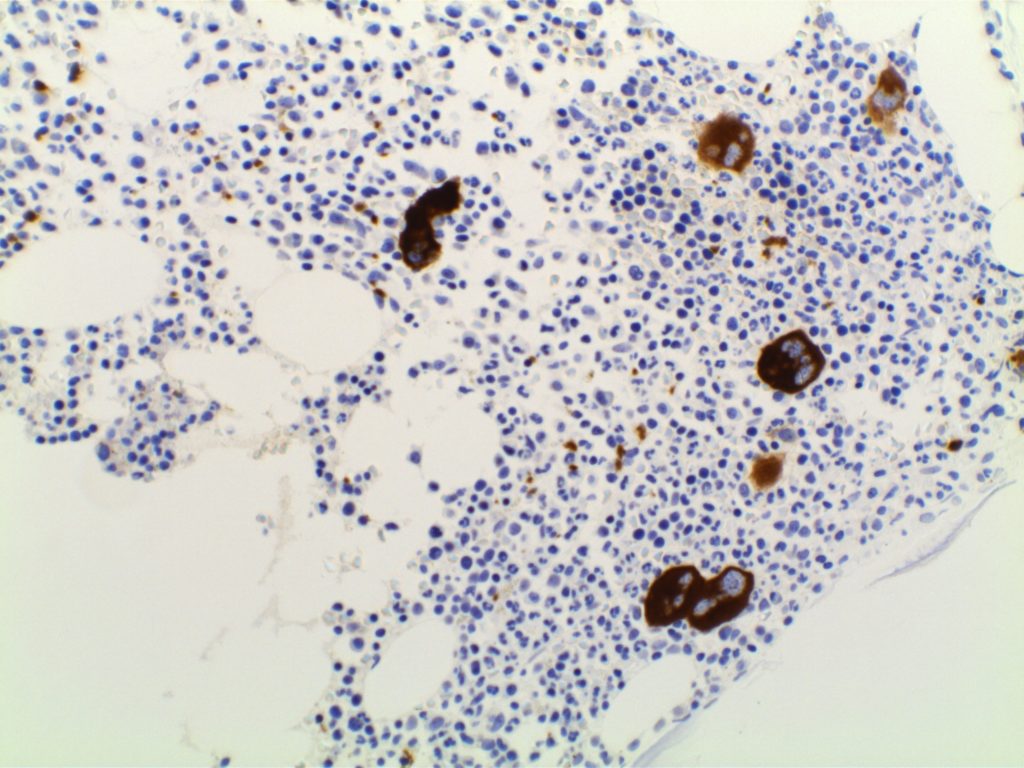
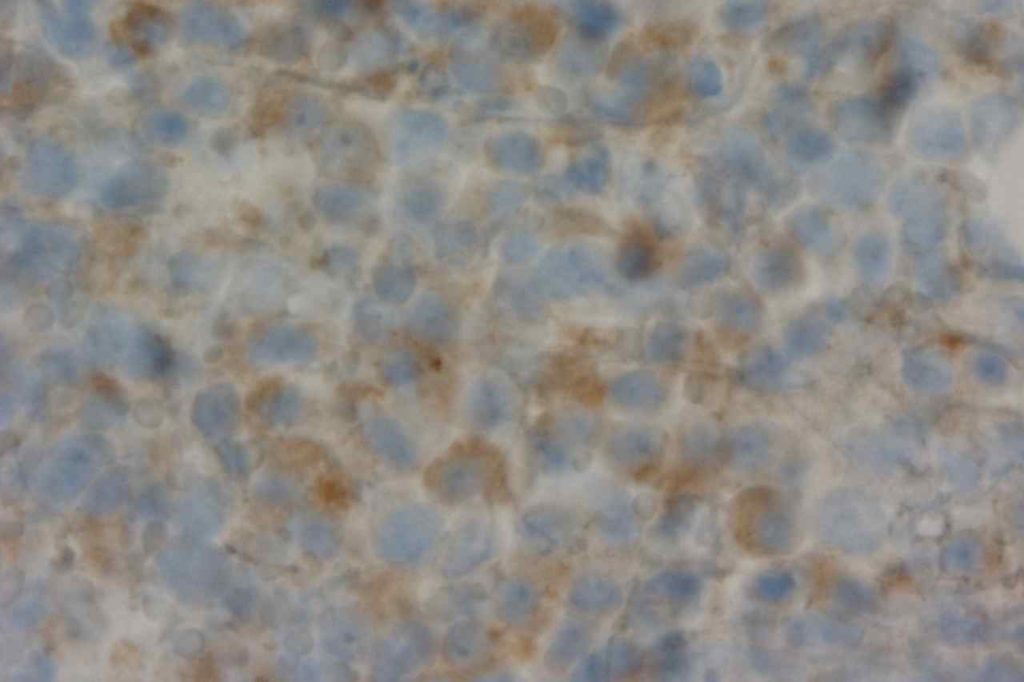
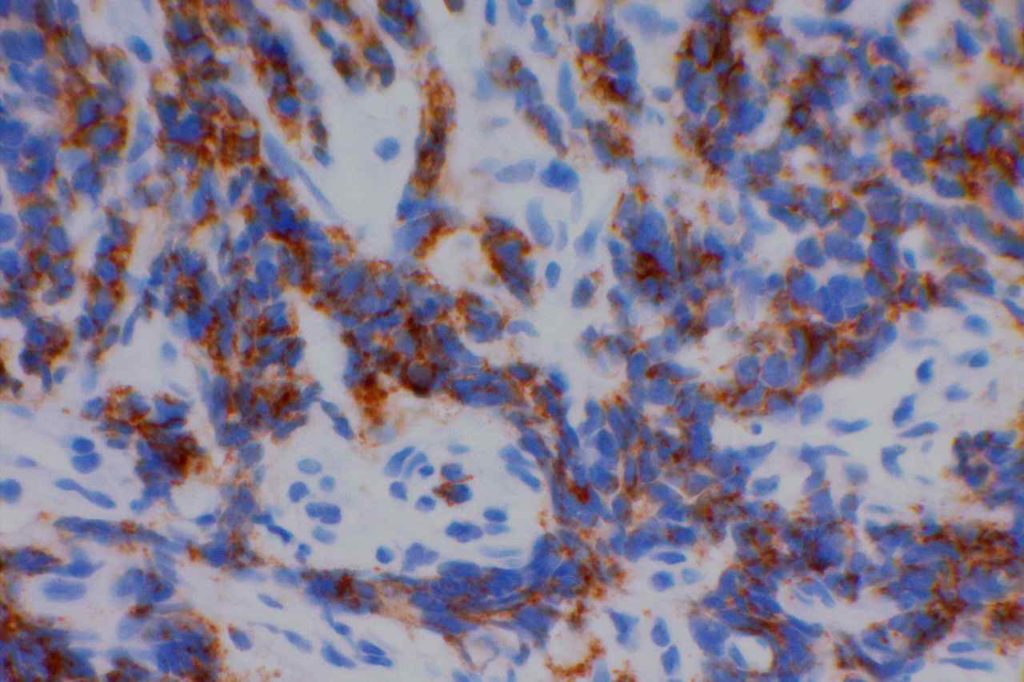
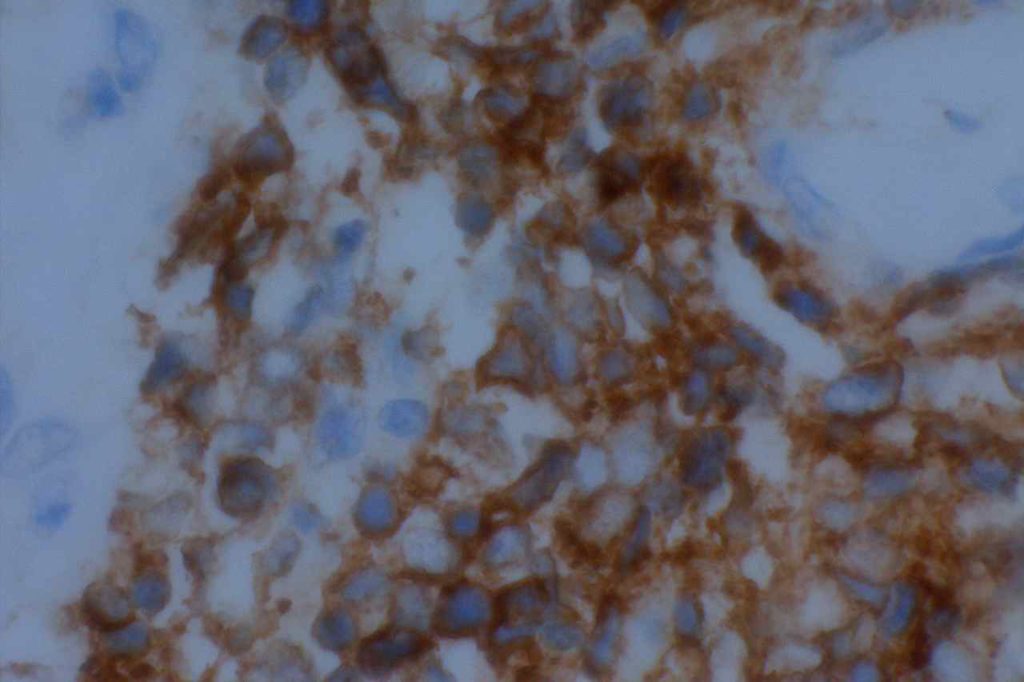
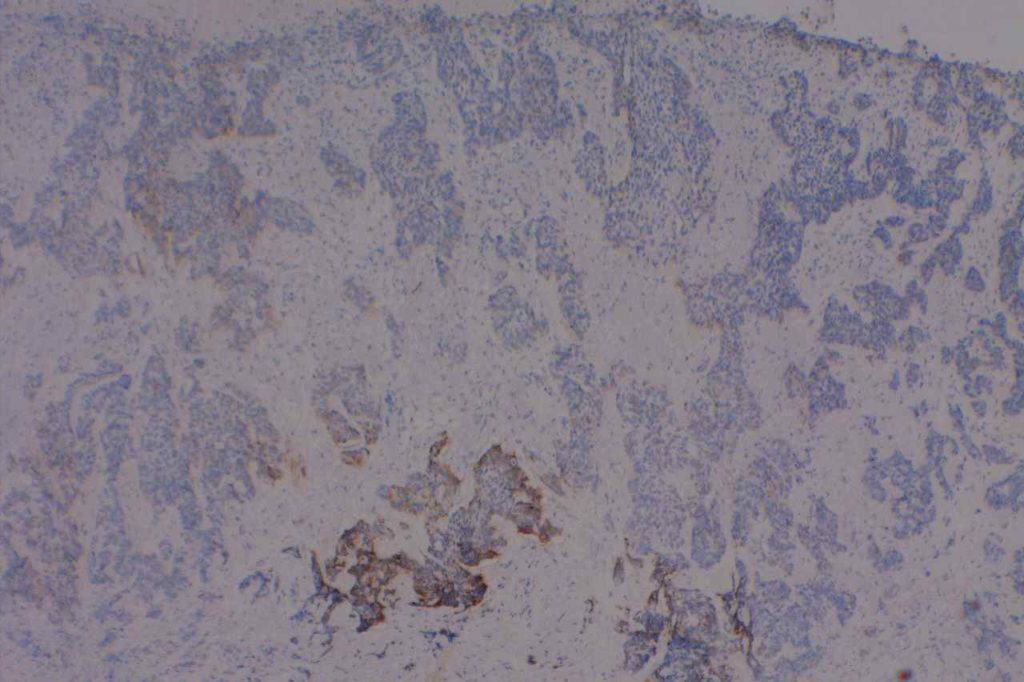
CD61 is a marker of megakaryocytes/platelets. The antigen is glycoprotein IIIa, and any cellular proliferation with megakaryocytic differentiation may express CD61. This marker has been found useful in bone marrow biopsies looking for identifying highlighting abnormal and micromegakaryocytes, which is found in some cases of myelodysplasia (MDS) and myeloproliferative neoplasms (MPN).
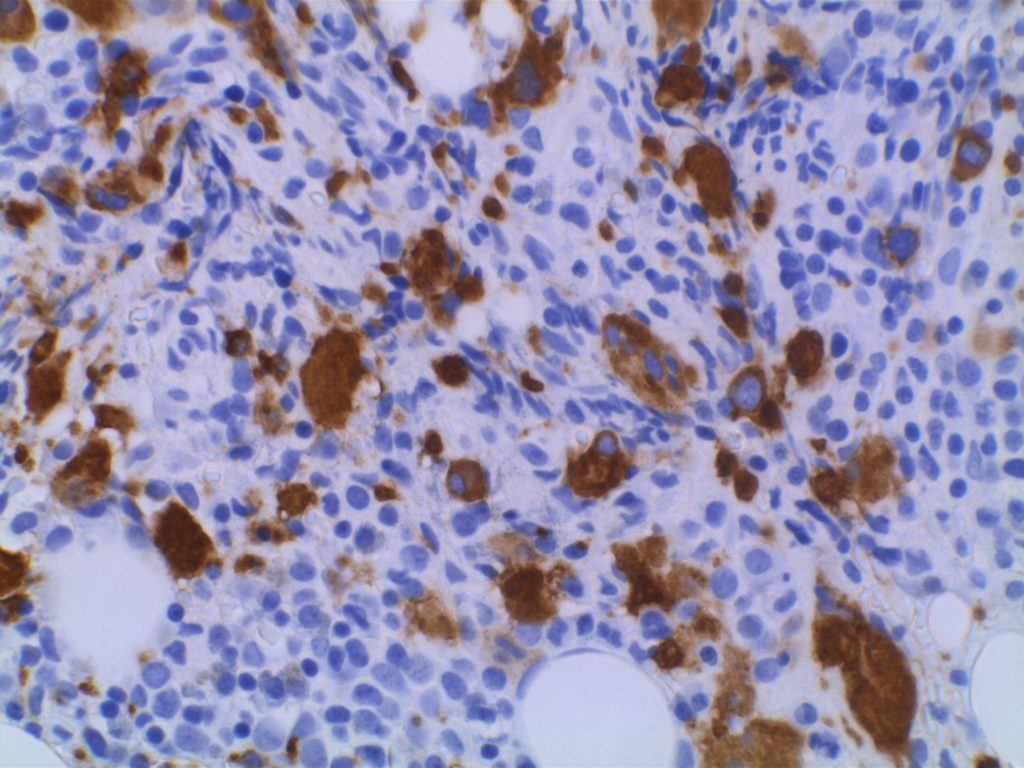
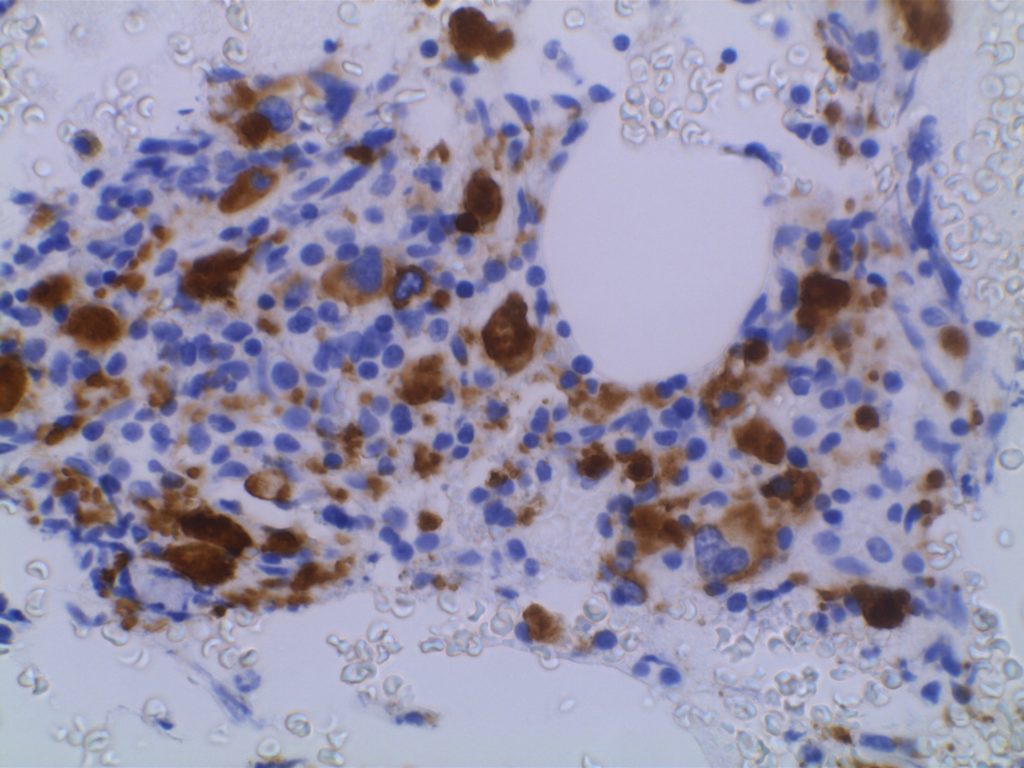
Some data suggests that at least 25% of the staining megakaryocytes should be micromegakaryocytes to have specificity for MDS (normal bone marrow <10% micromegakaryocytes). The opinion of some expert hematopathologists is that a significant proportion for MDS is >50% micromegakaryocytes.
Photomicrographs
CD61 expression in a normal bone marrow highlighting megakaryocytes.CD61 expression in a normal bone marrow highlighting megakaryocytes.CD61 expression in MDS (RAEB) with increased numbers of small and hypolobated megakaryocytes.CD61 expression in MDS (RAEB) with increased numbers of small and hypolobated megakaryocytes.
References
Quitmann H, Wagner S, Fischer R. Dysmegakaryopoiesis in myelodysplastic syndromes (MDS): an immunomorphometric study of bone marrow trephine biopsy specimens. Journal of Clinical Pathology. 1991.
Chuang SS, Li CY. Useful Panel of Antibodies for the Classification of Acute Leukemia by lmmunohistochemical Methods in Bone Marrow Trephine Biopsy Specimens. Am J Clin Pathol. 1997.
Jawad MD, Go RS, Reichard KK, Shi M. Increased Multinucleated Megakaryocytes as an Isolated Finding in Bone Marrow: A Rare Finding and Its Clinical Significance. Am J Clin Pathol. 2016;146: 561–566. doi:10.1093/ajcp/aqw144
FOX, S.B., LORENZEN, J., HERYET, A., JONES, M., GATTER, K.C. and MASON, D.Y. (1990), Megakaryocytes in myelodysplasia: an immunohistochemical study on bone marrow trephines. Histopathology, 17: 69–74. doi:10.1111/j.1365-2559.1990.tb00665.x
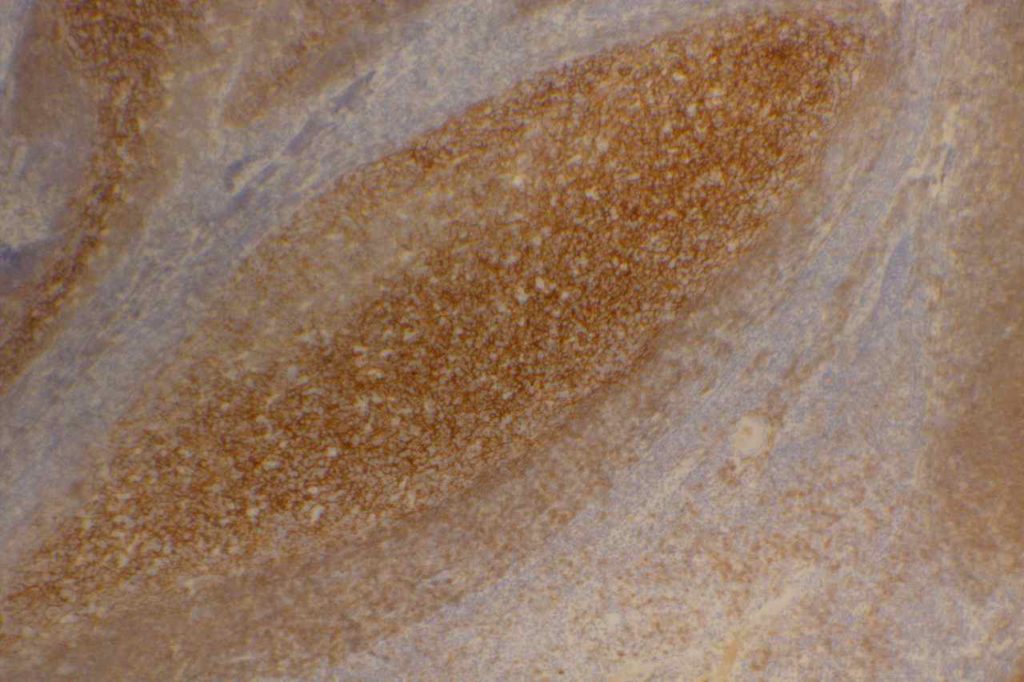
CD21 is a follicular dendritic cells (FDC) marker. It has a membranous staining pattern, but this is practically difficult to separate from a cytoplasmic pattern in lymphoid tissue. This stain is most often used as an “architectural” marker or aberrant patterns (nodular lymphocyte predominate Hodgkin lymphoma). There are some rare tumors of FDC, which will mark with CD21. CD21 may rarely mark normal B-cells, and strong expression of CD21 in CLL has been associated with a most aggressive disease course (unsure if this is by flow cytometry and/or IHC).
Follicular Lymphoma – It is also helpful to identify the expanded follicular dendritic meshwork in cases of follicular lymphoma (especially helpful in diagnostically challenging cases – i.e. identifying a follicular component in an otherwise diffuse process or in small needle biopsies where architecture may not be visible).
Angioimmunoblastic T-cell Lymphoma (AILT) – Extrafollicular dendritic cells in the paracortical region in associated with neoplastic T-cells and high endothelial venules is characteristic of AILT. CD21 is a helpful marker to highlights the follicular dendritic component in this process.
Marginal Zone Lymphoma – CD21 is useful in highlighting follicular colonization by marginal zone cells, which may be obscured by morphology alone.
CD21 Normal Expression Pattern
Follicular Dendritic Cells
Rare Normal B-cells
Rare cases of CLL
Generally thought of as a better follicular dendritic marker compared to CD23 (less sensitive)
Photomicrographs
CD21 highlighting the follicular dendritic meshwork in benign tonsil tissue.
MD DY-PW, BacSc F. A case of t (14; 18)-negative follicular lymphoma with atypical immunophenotype: usefulness of immunoarchitecture of Ki67, CD79a and follicular dendritic cell meshwork in making the diagnosis. Malaysian Journal of Pathology. 2014. p. 125-129.
Harris NL, Swerdlow SH, Jaffe ES,et al. FollicularLymphoma. In: Swerdlow SH, Campo E, Harris NL,Jaffe ES, Pileri SA, Stein H, Thiele J, VardimanJW,editors. WHO classication of tumours of haematopoietic and lymphoid tissues.4th ed. Lyon: IARC Press; 2008. p. 220–6.
Troxell ML, Schwartz EJ, van de Rijn M, Ross DT, Warnke RA, Higgins JP, et al. Follicular dendritic cell immunohistochemical markers in angioimmunoblastic T-cell lymphoma. Appl Immunohistochem Mol Morphol. 2005;13: 297–303.
Boyd SD, Natkunam Y, Allen JR, Warnke RA. Selective immunophenotyping for diagnosis of B-cell neoplasms: immunohistochemistry and flow cytometry strategies and results. Appl Immunohistochem Mol Morphol. 2013;21: 116–131. doi:10.1097/PAI.0b013e31825d550a
CD33 (gp67 and p67) is a specific hematopoietic marker, which is expressed in monocytes/macrophages, granulocyte precursors (decreases with maturation), mast cells, and dendritic cells.
Diagnostically, CD33 is helpful in differentiating myeloid tumors for lymphoid neoplasms. Myelomonocytic and monoblastic leukemias may mark with CD33, but are usually negative for myeloperoxidase (MPO). Hematodermic neoplasm is also negative for CD33.
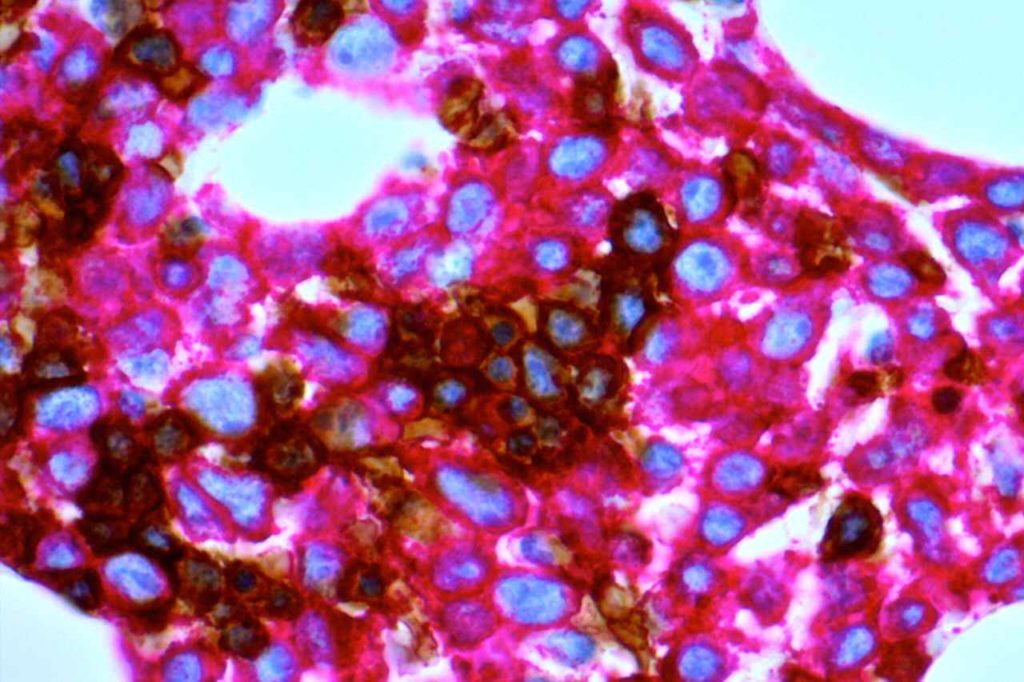
CD43 is a pan T-cell marker, which is also expressed in myeloid (granulocytic) sarcomas and some B-cell lymphomas. CD43 is aberrantly expressed in a number of B-cell lymphomas (expression is highly correlated with CD5), but this marker is most helpful in cases of marginal zone lymphoma when flow cytometry is not performed (i.e. usually small mucosal biopsies). These cases may be difficult to differentiate from lymphoid hyperplasia. Approximately 50% of cases of marginal zone lymphoma will express CD43. Negativity for CD43 does not exclude the diagnosis, and additional molecular testing may be helpful to identify these cases.
Lee et. al identified normal co-expression of CD43 (strong expression) in perifolliuclar B-cells within submucosal lymphoid tissue from terminal ileum biopsies. Therefore, CD43 co-expression on terminal ileum biopsies should NOT be used as a criterion alone to favor a diagnosis of MALT lymphoma.
The main take home point is that CD43 is a good marker, which is helpful, but there is lack a specificty and one should understand the stain performance in the diagnostic setting. In the workup of a mature B cell lymphoma, CD43 (like CD5) should be compared against CD3 and CD20 staining.
CD43 Expression in Non-Hodgkin Lymphoma (Lai R., et. al. N=742 cases)
In the skin CD43 marked >95% of cases of granulocytic sarcoma (leukemia cutis). Other non-T cell lesions which may stain with CD43 include: AML, hemangioma, Langerhans cell histiocytosis, mast cell disease and plasmacytoma.
Photomicrographs
Aberrant CD43 expression in mantle cell lymphoma.
References
Lai, R., Weiss, L. M., Chang, K. L., & Arber, D. A. (1999). Frequency of CD43 expression in non-Hodgkin lymphoma. A survey of 742 cases and further characterization of rare CD43+ follicular lymphomas. American Journal of Clinical Pathology, 111(4), 488–494.
Treasure, J., Lane, A., Jones, D. B., & Wright, D. H. (1992). CD43 expression in B cell lymphoma. Journal of Clinical Pathology, 45(11), 1018–1022.
Cronin, D. M. P., George, T. I., & Sundram, U. N. (2009). An updated approach to the diagnosis of myeloid leukemia cutis. American Journal of Clinical Pathology, 132(1), 101–110. doi:10.1309/AJCP6GR8BDEXPKHR
Jung G, Eisenmann J-C, Thiébault S, Hénon P. Cell surface CD43 determination improves diagnostic precision in late B-cell diseases. Br J Haematol. 2003;120: 496–499.
Lee P-S, Beneck D, Weisberger J, Gorczyca W. Coexpression of CD43 by benign B cells in the terminal ileum. Appl Immunohistochem Mol Morphol. 2005;13: 138–141.
Diagnostic Immunohistochemistry: Theranostic and Genomic Applications [edited by] David J. Dabbs. 3rd Edition. pp. 165.
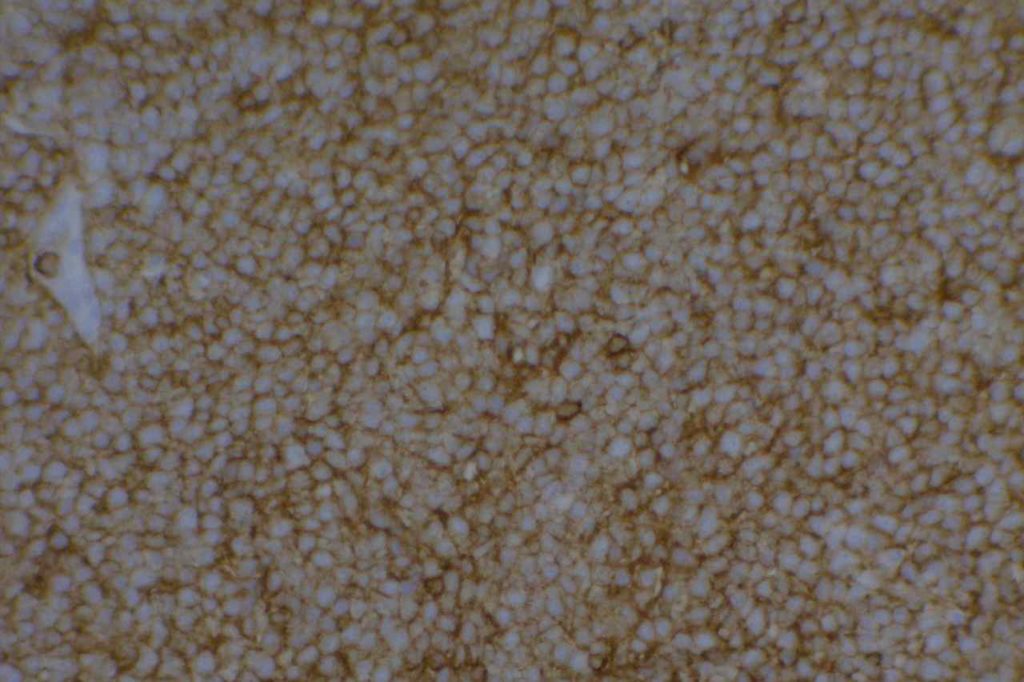
CD45 (LCA) is also known as leukocyte common antigen (LCA). It is a sensitive marker for lymphoid cells. In the most general form it is often used as part of a panel for undifferentiated tumors or so-called “small round blue cell tumors.” Such a screening panel usually includes:
Loss of CD45 expression in Hodgkin cells in a case of nodular sclerosing classical Hodgkin lymphoma (CHL).Strong diffuse expression of CD45 in a non-Hodgkin lymphoma.
References
Wick, MR. “Immunohistochemical approaches to the diagnosis of undifferentiated malignant tumor.”Annals of Diagnostic Pathology12(2008):72-84.
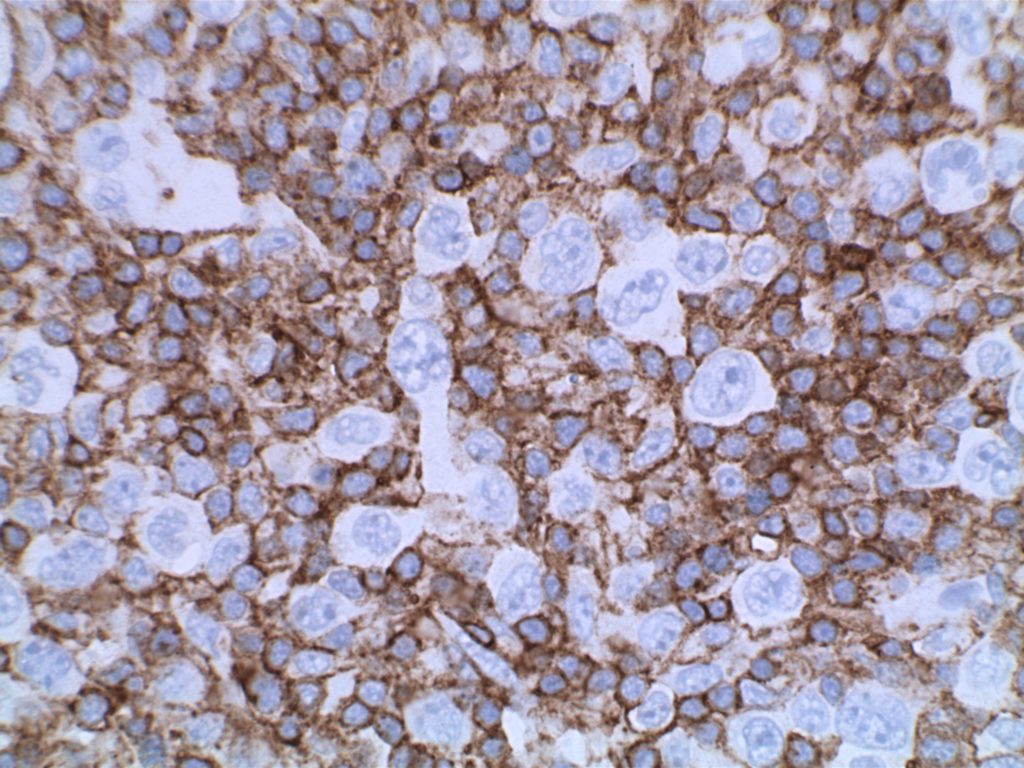
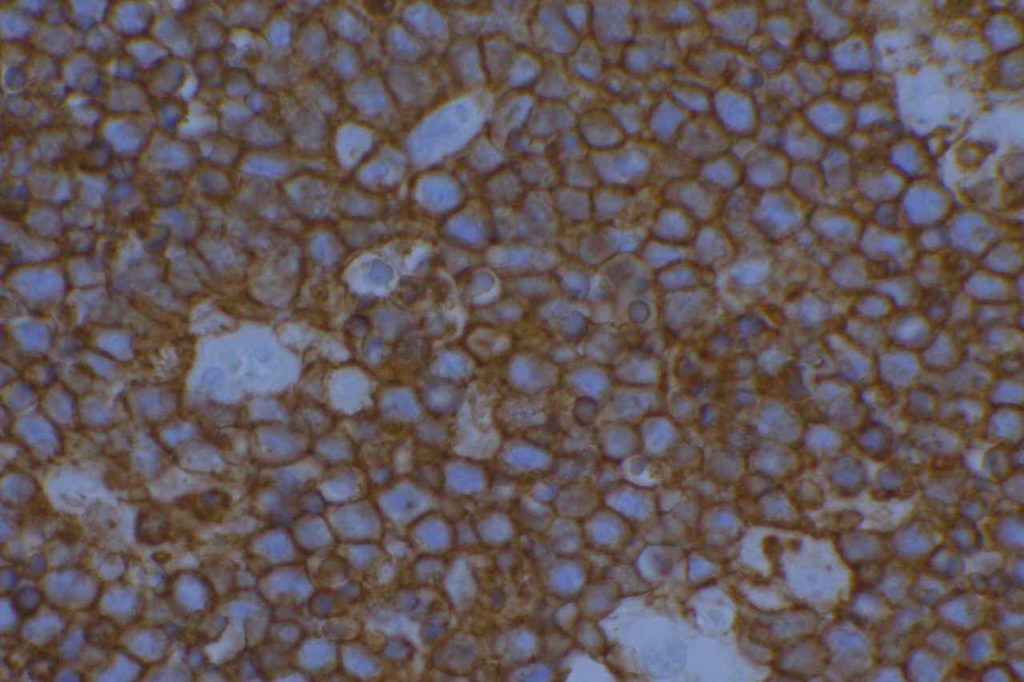
CD56 (NCAM – neural-cell adhesion molecule) is expressed on the surface of neuroendocrine epithelial cells, some Schwann cells, and some neuroendocrine tumors. In undifferentiated tumors, CD56 can be used as a screening marker for neuroendocrine differentiation. It appears to be more sensitive than synaptophysin or chromogranin A in most situations, but Ishida, et. al found CD56 to be the least sensitive of the three in neuroendocrine carcinomas of the stomach (47% compared to 94% and 86% for synaptophysin and chromogranin A, respectively).
CD56 also marks a subset of hematopoeitic and gonadal-stromal cells. Expression of CD56 alone should does not have significant specificity.
CD56 Sensitivity for high grade neuroendocrine tumors
Stomach – 47% (Ishida, et. al)
Esophagus – 93% (Huang, et. al)
Lung – >90% (Travis, et. al)
Hematopathology
Marks approximately ~20-50% of cases of leukemia cutis.
Plasma cell myeloma – Abnormal plasma cells will often express CD56 in addition to CD138, and can be very helpful when flow cytometry and kappa/lambda studies fail to identify an abnormal plasma cell population.
Basal cell carcinomas (BCC) show strong membrane and less intense cytoplasmic staining with CD56. Important not to use with the differential diagnosis of merkel cell carcinoma. Squamous cell carcinomas (SCC) do not express CD56, and in the BCC vs. SCC differential CD56 may be helpful.
CD56 Expression Pattern – Other
BM Osteoblasts
Neuroendocrine Neoplasms
Basal cell carcinoma
Photomicrographs
CD56 expression in a NK-cell lymphoma.CD56 expression in small cell carcinoma.CD56 expression in Merkel cell carcinomaCD56 expression in a subset basal cell carcinoma tumor cells.
References
Cronin DMP, George TI, Sundram UN. An updated approach to the diagnosis of myeloid leukemia cutis. Am J Clin Pathol. 2009;132: 101–110. doi:10.1309/AJCP6GR8BDEXPKHR
Wick MR. Immunohistochemical approaches to the diagnosis of undifferentiated malignant tumors. Annals of Diagnostic Pathology. 2008;12: 72–84. doi:10.1016/j.anndiagpath.2007.10.003
Ishida M, Sekine S, Fukagawa T, Ohashi M, Morita S, Taniguchi H, et al. Neuroendocrine carcinoma of the stomach: morphologic and immunohistochemical characteristics and prognosis. Am J Surg Pathol. 2013;37: 949–959. doi:10.1097/PAS.0b013e31828ff59d
Huang Q, Wu H, Nie L, Shi J, Lebenthal A, Chen J, et al. Primary high-grade neuroendocrine carcinoma of the esophagus: a clinicopathologic and immunohistochemical study of 42 resection cases. Am J Surg Pathol. 2013;37: 467–483. doi:10.1097/PAS.0b013e31826d2639
Cronin DMP, George TI, Reichard KK, Sundram UN. Immunophenotypic analysis of myeloperoxidase-negative leukemia cutis and blastic plasmacytoid dendritic cell neoplasm. Am J Clin Pathol. 2012;137: 367–376. doi:10.1309/AJCP9IS9KFSVWKGH
Bénet C, Gomez A, Aguilar C, Delattre C, Vergier B, Beylot-Barry M, et al. Histologic and immunohistologic characterization of skin localization of myeloid disorders: a study of 173 cases. Am J Clin Pathol. 2011;135: 278–290. doi:10.1309/AJCPFMNYCVPDEND0
Joshi R, Horncastle D, Elderfield K, Lampert I, Rahemtulla A, Naresh KN. Bone marrow trephine combined with immunohistochemistry is superior to bone marrow aspirate in follow-up of myeloma patients. J Clin Pathol. 2008;61: 213–216. doi:10.1136/jcp.2007.049130
Seegmiller AC, Xu Y, McKenna RW, Karandikar NJ. Immunophenotypic differentiation between neoplastic plasma cells in mature B-cell lymphoma vs plasma cell myeloma. Am J Clin Pathol. 2007;127: 176–181. doi:10.1309/5EL22BH45PHUPM8P
BELJAARDS RC, KIRTSCHIG G, BOORSMA DM. Expression of neural cell adhesion molecule (CD56) in basal and squamous cell carcinoma. Dermatol Surg. 2008;34: 1577–1579. doi:10.1111/j.1524-4725.2008.34327.x
Herling M, Jones D. CD4+/CD56+ hematodermic tumor: the features of an evolving entity and its relationship to dendritic cells. Am J Clin Pathol. 2007;127: 687–700. doi:10.1309/FY6PK436NBK0RYD4
Travis WD. Update on small cell carcinoma and its differentiation from squamous cell carcinoma and other non-small cell carcinomas. Mod Pathol. Nature Publishing Group; 2012;25: S18–S30. doi:10.1038/modpathol.2011.150
CD68 (gp110) is a glycosylated lysosomal transmembrane glycoprotein, which is normally expressed on monocytes, macrophages, dendritic cells, neutrophils, basophils, myeloid progenitor cells, mast cells, activated T-cells, and a subset of blasts. The staining pattern is generally cytoplasmic. Almost all MPO+ bone marrow cells will express CD68.
In the setting of leukemia cutis, CD68 was expressed in >95% of cases (Benet, et. al). Typically, CD68 is used to identify histiocytes. Unfortunately, CD68 lacks specificity and the morphologic differential diagnosis overlaps in many situations, and use as part of a larger panel yields more specific results.
CD68R (PGM-1) is one of the epitopes of CD68, and appears to be the most monocyte specific marker of the CD68 family. Expression in monocytic differentiated AMLs is reported to be 92-94% (Rollins-Raval, et. al)
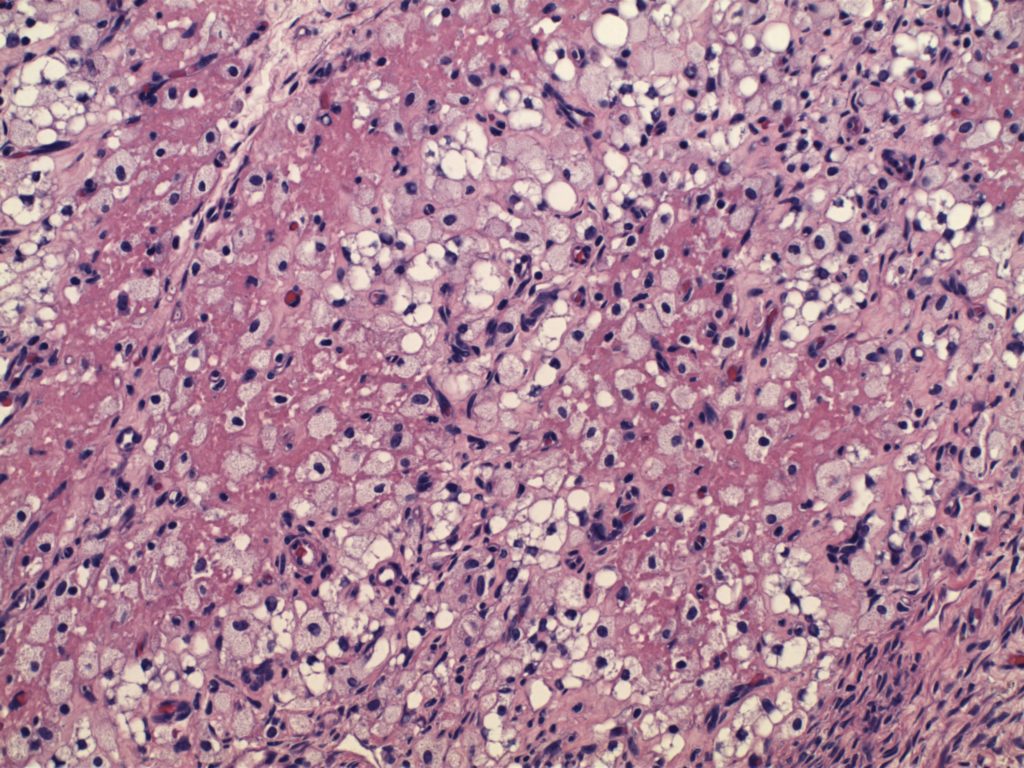
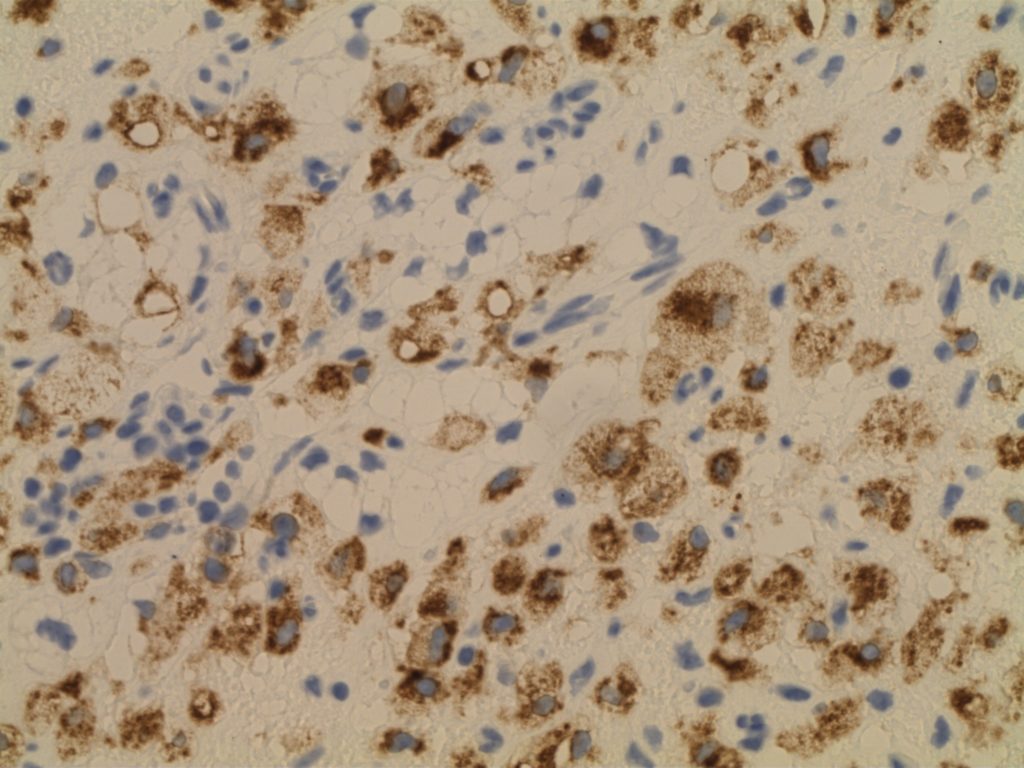
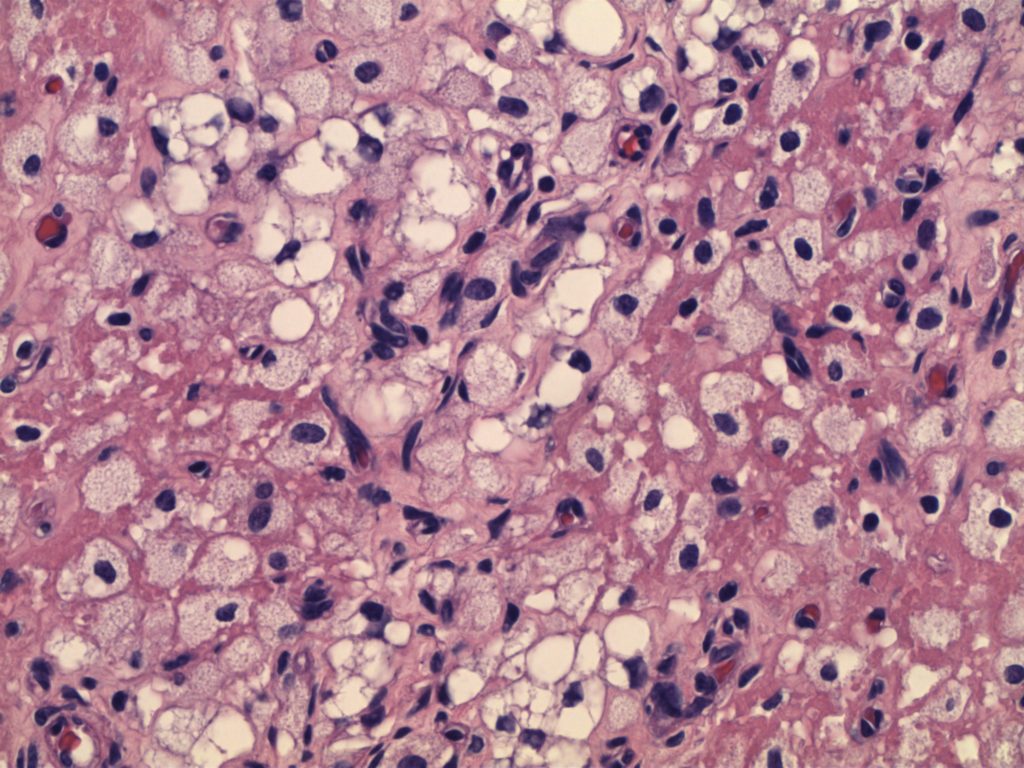
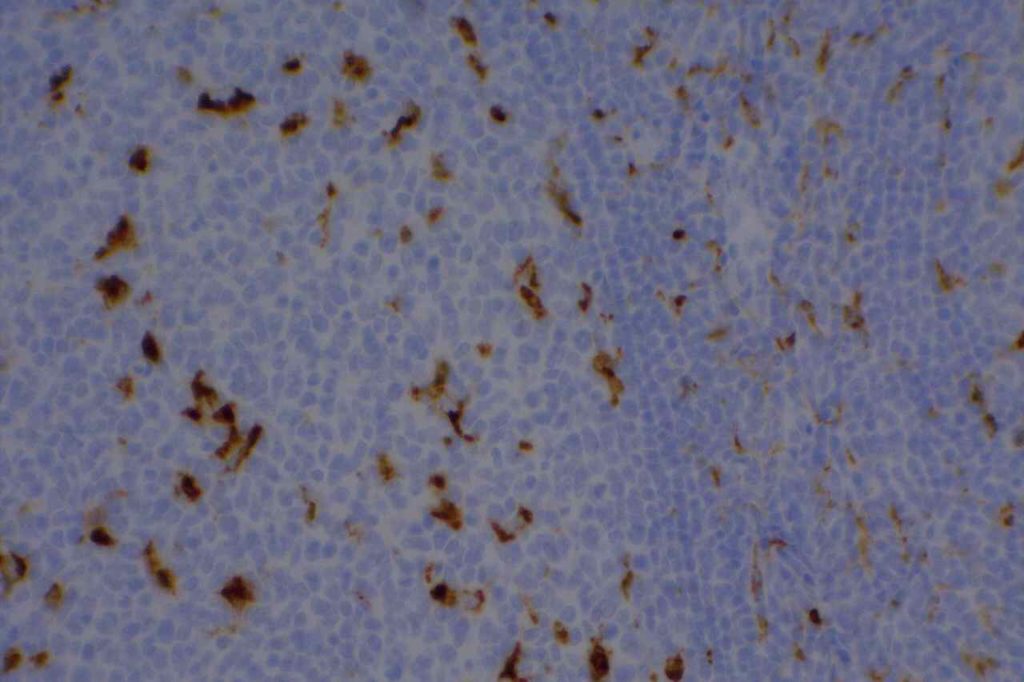
Photomicrographs
H&E section of ovary showing histiocytes.CD68 staining histiocytes in ovarian parenchyma with physiologic type changes.High power view of ovary parenchyma with histiocytes (physiologic changes).CD68 highlighting scattered macrophages in benign tonsil.
Bénet C, Gomez A, Aguilar C, Delattre C, Vergier B, Beylot-Barry M, et al. Histologic and immunohistologic characterization of skin localization of myeloid disorders: a study of 173 cases. Am J Clin Pathol. 2011;135: 278–290. doi:10.1309/AJCPFMNYCVPDEND0
Cronin DMP, George TI, Sundram UN. An updated approach to the diagnosis of myeloid leukemia cutis. Am J Clin Pathol. 2009;132: 101–110. doi:10.1309/AJCP6GR8BDEXPKHR
Rollins-Raval MA, Roth CG. The value of immunohistochemistry for CD14, CD123, CD33, myeloperoxidase and CD68R in the diagnosis of acute and chronic myelomonocytic leukaemias. Histopathology. 2012;60: 933–942. doi:10.1111/j.1365-2559.2012.04175.x
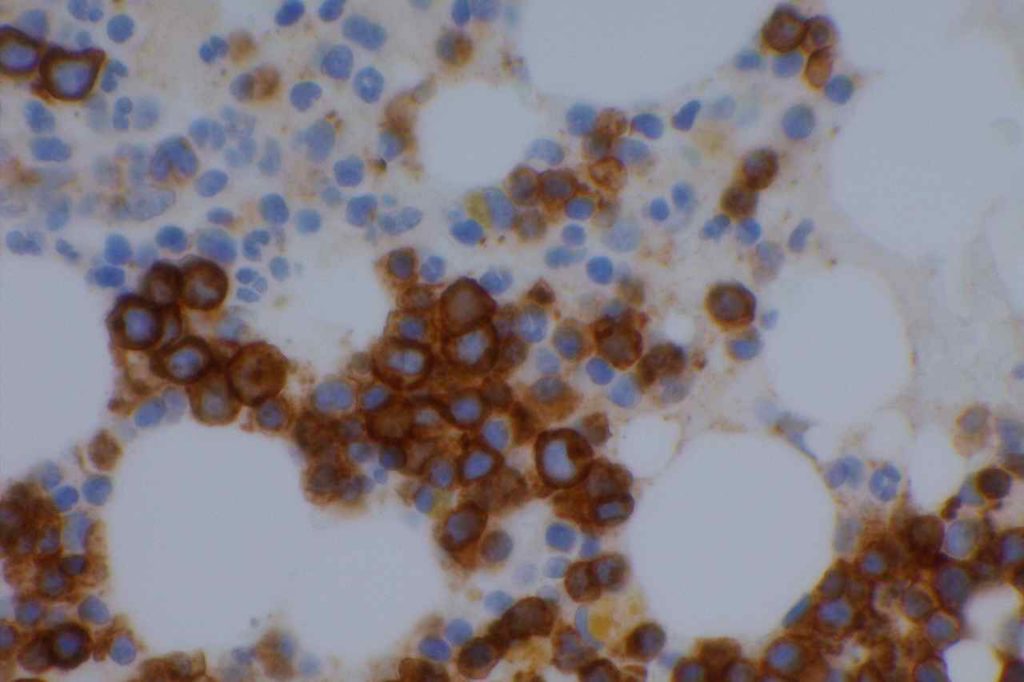
CD71 is one of the most useful, but least used antibodies in hematopathology. CD71 is an integral membrane protein, which is involved in the uptake of the transferrin-iron complex. Immunoreactivity is restricted to erythroid precursors with a membranous and cytoplasmic stain pattern.
Previously there have been other erythroid markers, but they have been difficult to interpret because they stain all RBCs and precursors. CD71 stains immature erythroid precursors, which are nucleated, and is not significantly expressed in mature RBCs. The utility of CD71 is to help differentiate between normoblasts and myeloblasts in bone marrow specimens. This is especially powerful when combined with CD34 (sensitive/not specific myeloblast marker) on a dual staining IHC platform (red and DAB chromogens).
CD71 can be a particularly useful tool to help accurately characterize immature cellular elements in bone marrow specimens, and decrease misidentification of normoblasts for myeloblasts and/or ALIP. E-Cadherin will also stain immature erythroid precursors (usually in a dimmer pattern compared to CD71).
Utilization of CD71 in gestational pathology has found it to be helpful to identify nucleated red blood cells (NRBCs) in partial molar pregnancies and spontaneous abortions in contrast to complete moles (absence of NRBCs).
Dim staining is expected in lymphoid cells (significantly different from nucleated red cell precursors), which can serve as a nice control (e.g. tonsil tissue).
Photomicrographs
Lymphoid aggregate with dim CD71 expression (erythroid precursors at the periphery). Can be useful as a control (e.g. tonsil).CD34 (red) and CD71 (brown) double stain in a case of acute myelogenous leukemia (AML).CD71 highlighting erythroid precursors in a normal bone marrow sample.
References
Marsee, D. K., Pinkus, G. S., & Yu, H. (2010). CD71 (transferrin receptor): an effective marker for erythroid precursors in bone marrow biopsy specimens. American Journal of Clinical Pathology, 134(3), 429–435. doi:10.1309/AJCPCRK3MOAOJ6AT
Dong, H. Y., Wilkes, S., & Yang, H. (2011). CD71 is Selectively and Ubiquitously Expressed at High Levels in Erythroid Precursors of All Maturation Stages: A Comparative Immunochemical Study With Glycophorin A and Hemoglobin A. The American journal of surgical pathology, 35(5), 723–732. doi:10.1097/PAS.0b013e31821247a8
Luchini C, Parcesepe P, Nottegar A, Parolini C, Mafficini A, Remo A, et al. CD71 in Gestational Pathology: A Versatile Immunohistochemical Marker With New Possible Applications. Appl Immunohistochem Mol Morphol. 2016;24: 215–220. doi:10.1097/PAI.0000000000000175
Acs G, LiVolsi VA. Loss of membrane expression of E-cadherin in leukemic erythroblasts. Arch Pathol Lab Med. 2001;125: 198–201. doi:10.1043/0003-9985(2001)125<0198:LOMEOE>2.0.CO;2
Sadahira Y, Kanzaki A, Wada H, Yawata Y. Immunohistochemical identification of erythroid precursors in paraffin embedded bone marrow sections: spectrin is a superior marker to glycophorin. J Clin Pathol. 1999;52: 919–921.
CD79a (MB1) is a B-cell marker with a wider range of positivity in the B-cell development spectrum compared to CD20 (mature B-cell phenotype). CD79a may be expressed on malignant precursor B-cells and terminally differentiated B-cells (PAX-5 is not expressed in terminally differentiated B-cells). Please note that in the setting of ALL, CD79a is not lineage specific, and up to 50% of T-ALL cases express CD79a. AML cases with t(8;21) may also show CD79a expression (along with CD19, CD20, and TdT).
CD99 (MIC-2 or p30/32) has an unknown function, but has been found to be expressed in vitally all cases of primitive neuroectodermal tumors (PNETs) and Ewing sarcoma. The specificity is more limited and may be seen in alveolar rhabdomyosarcomas (15%), ALLs (90%), neuroendocrine carcinomas (20%), melanomas, etc. Therefore, CD99 should not be interpreted alone, and is best used as part of a panel (e.g. AE1/AE3, desmin, S-100, and CD45 in an undifferentiated small round blue cell tumor situation).
Note: CD99 was originally described as being sensitive and “specific” for PNETs. However, expression in a variety of other tumors (including tumors with similar morphologies to PNETs) were also found to have expression (at least in a subset of cases). Sensitivity of “new” IHC markers can be determined with a fair degree of accuracy using tissue arrays and large tumor libraries, but it usually takes time with efforts from many different laboratories to fully characterize the “specificity” of a marker. This should always be taken into consideration when relying heavily on a “new” marker for diagnostic significance.
Rao, N., Colby, T. V., Falconieri, G., Cohen, H., Moran, C. A., & Suster, S. (2013). Intrapulmonary solitary fibrous tumors: clinicopathologic and immunohistochemical study of 24 cases. The American Journal of Surgical Pathology, 37(2), 155–166. doi:10.1097/PAS.0b013e31826a92f5