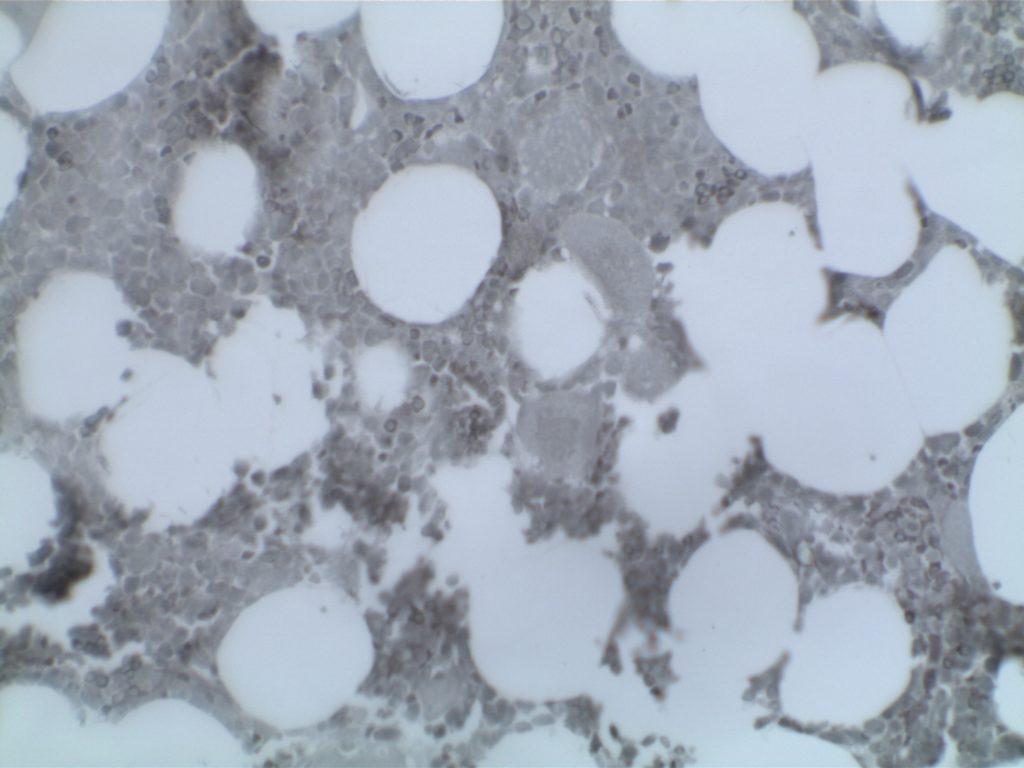
The use of immunohistochemistry (IHC) in many of the myeloproliferative neoplasms is limited. Identifying an increased blast population is one of the most useful, and may indicate a more aggressive course or transformation to acute leukemia. Helpful IHC markers may include:
CD117 is a specific myeloid marker, and marks a subset of myeloblasts. The expression is dim, and one often must look at 20-40X to clearly see expression. Mast cells (fried egg looking cell) will have very strong expression.
CD71 marks nucleated erythroid cells. This may be helpful in quantitating and differentiating erythroid cells from myeloid cells. This marker may be set-up as a double stain with CD34.
In the setting of hematopoietic cells, E-Cadherin marks immature erythroid cells. Like CD71, E-Cadherin may be useful to differentiate immature erythroid cells from immature myeloid cells.
TdT is a sensitive lymphoblast (~95%) marker. It is not entirely specific for lymphoblasts, but other markers can help clarify diagnostic difficulties (B and T-cell markers).
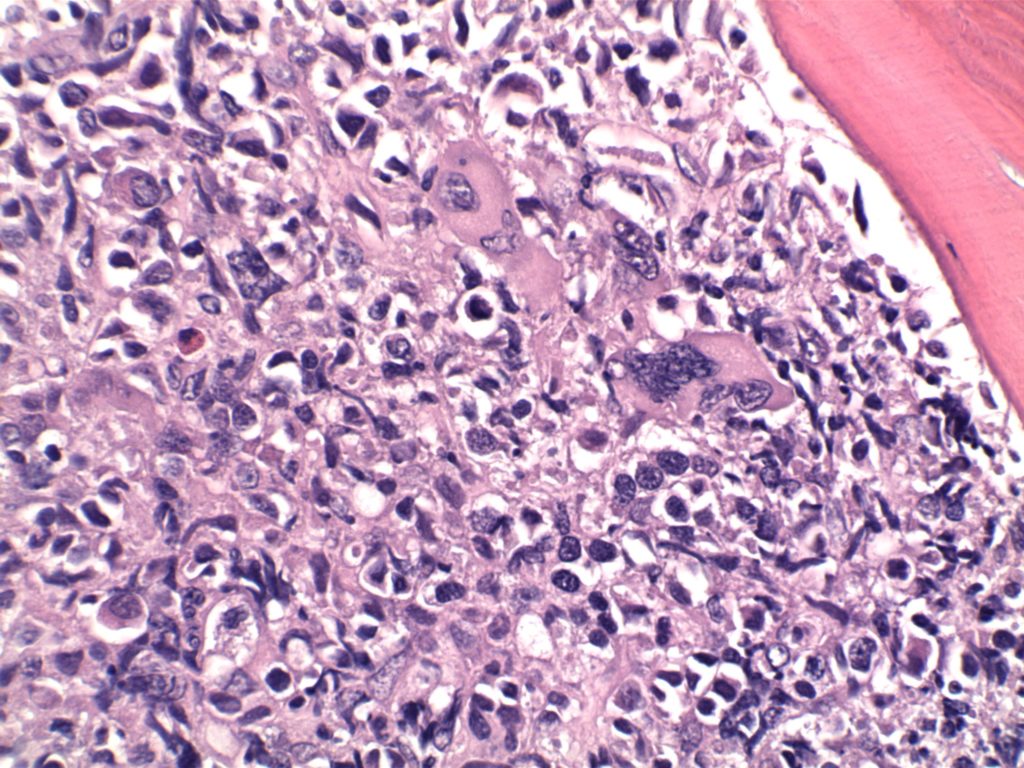
Mastocytosis is a clonal (neoplastic) proliferation of mast cells. It can be a heterogeneous disorder ranging from skin lesion, which spontaneously regress, to aggressive systemic disease with a short survival. Mastocytosis is divided into two generalized categories: cutaneous mastocytosis (CM) and systemic mastocytosis (SM). CM is limited strictly to the skin, but SM has at least one extracutaneous organ involved (+/- skin involvement).
In SM the bone marrow is almost always involved. Approximately 50% of SM patients will have skin involvement.
Strongly reactive (must be used in combination with MPO)
MPO
Negative
Tryptase
Positive, not specific. Positivity of spindle cells in the bone marrow (BM) is considered specific for mast cells. Positivity of round cells in the BM may represent one of three entities: (1) mast cells (CD117+, chymase +), (2) neoplastic basophils, or (3) AML.
Chymase
Subset Positive (highly specific but not sensitive)
Expressed in a subset of neoplastic mast cells (specific). Must differentiate from T-cells. Commonly expressed in neoplastic mast cells involving the GI tract.
The use of immunohistochemistry (IHC) in many of the myeloproliferative neoplasms is limited. Identifying an increased blast population is one of the most useful, and may indicate a more aggressive course or transformation to acute leukemia. Helpful IHC markers may include:
CD117 is a specific myeloid marker, and marks a subset of myeloblasts. The expression is dim, and one often must look at 20-40X to clearly see expression. Mast cells (fried egg looking cell) will have very strong expression.
CD71 marks nucleated erythroid cells. This may be helpful in quantitating and differentiating erythroid cells from myeloid cells. This marker may be set-up as a double stain with CD34.
In the setting of hematopoietic cells, E-Cadherin marks immature erythroid cells. Like CD71, E-Cadherin may be useful to differentiate immature erythroid cells from immature myeloid cells.
TdT is a sensitive lymphoblast (~95%) marker. It is not entirely specific for lymphoblasts, but other markers can help clarify diagnostic difficulties (B and T-cell markers).
Does not meet the WHO criteria for another myeloid neoplasm
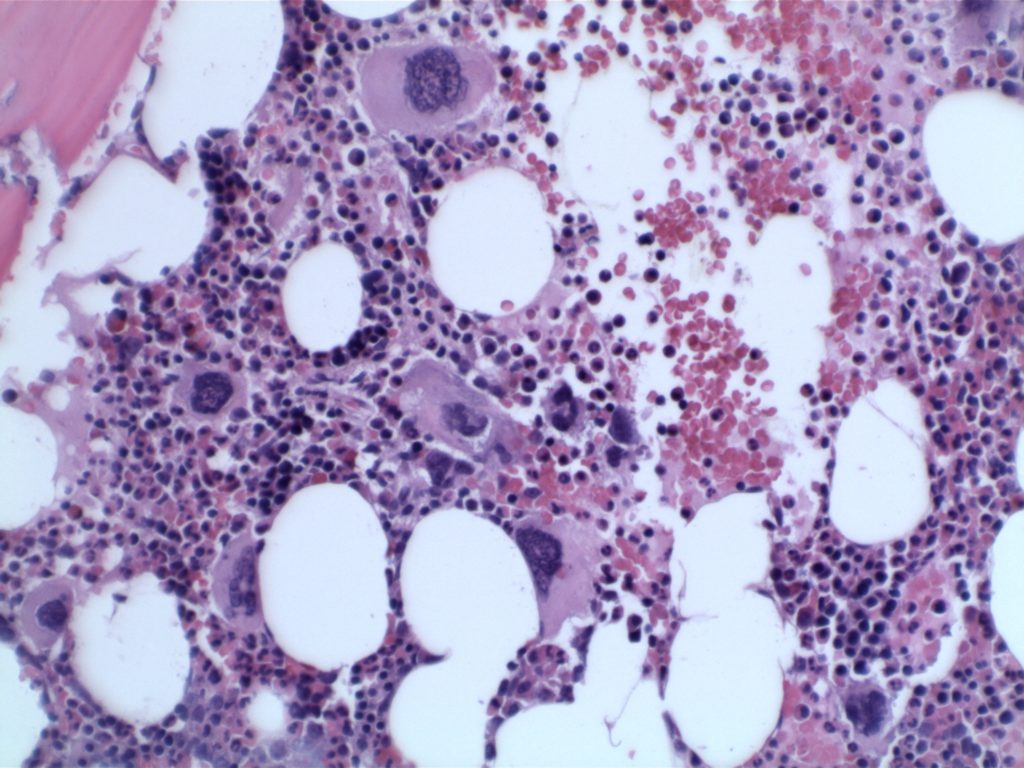
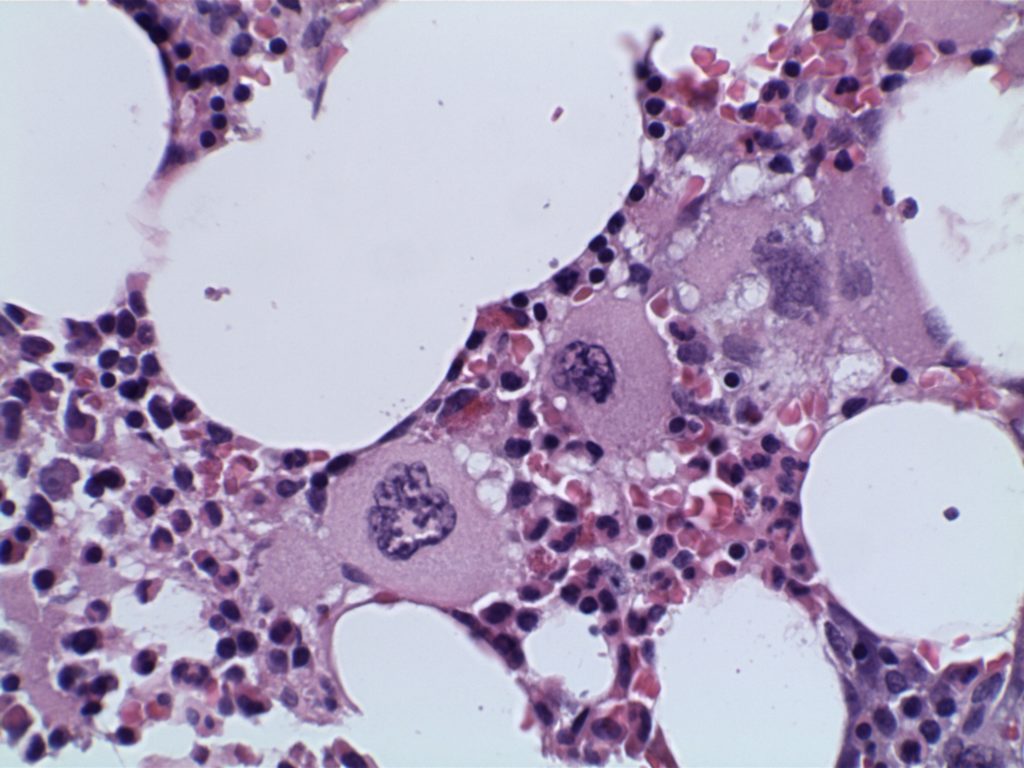
BM biopsy showing megakaryocytic proliferation
Enlarged mature megakaryocytes
Hyperlobated nuclei (not as pleomorphic or bizzare as in PMF)
Granulopoiesis and erythropoiesis is not increased or left shifted
No more than MF1 reticulin fibrosis
Minor Criteria
Evidence of a clonal marker or exclusion of reactive thrombocytosis
Diagnosis of ET is confirmed by all four major criteria, or if there is no evidence of a JAK2, CALR, or MPL mutation (major criterion #2), then the presence of the minor criterion.
Frequency of Molecular Abnormalities
JAK2 – 63% (V617F mutation)
CALR – 18%
MPL – 2-3%
Overall, approximately 83% of cases of ET have either a JAK2, CALR, or MPL mutation (n=79).
The use of immunohistochemistry (IHC) in many of the myeloproliferative neoplasms is limited. Identifying an increased blast population is one of the most useful, and may indicate a more aggressive course or transformation to acute leukemia. Helpful IHC markers may include:
CD117 is a specific myeloid marker, and marks a subset of myeloblasts. The expression is dim, and one often must look at 20-40X to clearly see expression. Mast cells (fried egg looking cell) will have very strong expression.
CD71 marks nucleated erythroid cells. This may be helpful in quantitating and differentiating erythroid cells from myeloid cells. This marker may be set-up as a double stain with CD34.
In the setting of hematopoietic cells, E-Cadherin marks immature erythroid cells. Like CD71, E-Cadherin may be useful to differentiate immature erythroid cells from immature myeloid cells.
TdT is a sensitive lymphoblast (~95%) marker. It is not entirely specific for lymphoblasts, but other markers can help clarify diagnostic difficulties (B and T-cell markers).
Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127: 2391–2405. doi:10.1182/blood-2016-03-643544
Kim SY, Im K, Park SN, Kwon J, Kim J-A, Lee DS. CALR, JAK2, and MPL mutation profiles in patients with four different subtypes of myeloproliferative neoplasms: primary myelofibrosis, essential thrombocythemia, polycythemia vera, and myeloproliferative neoplasm, unclassifiable. Am J Clin Pathol. 2015;143: 635–644. doi:10.1309/AJCPUAAC16LIWZMM
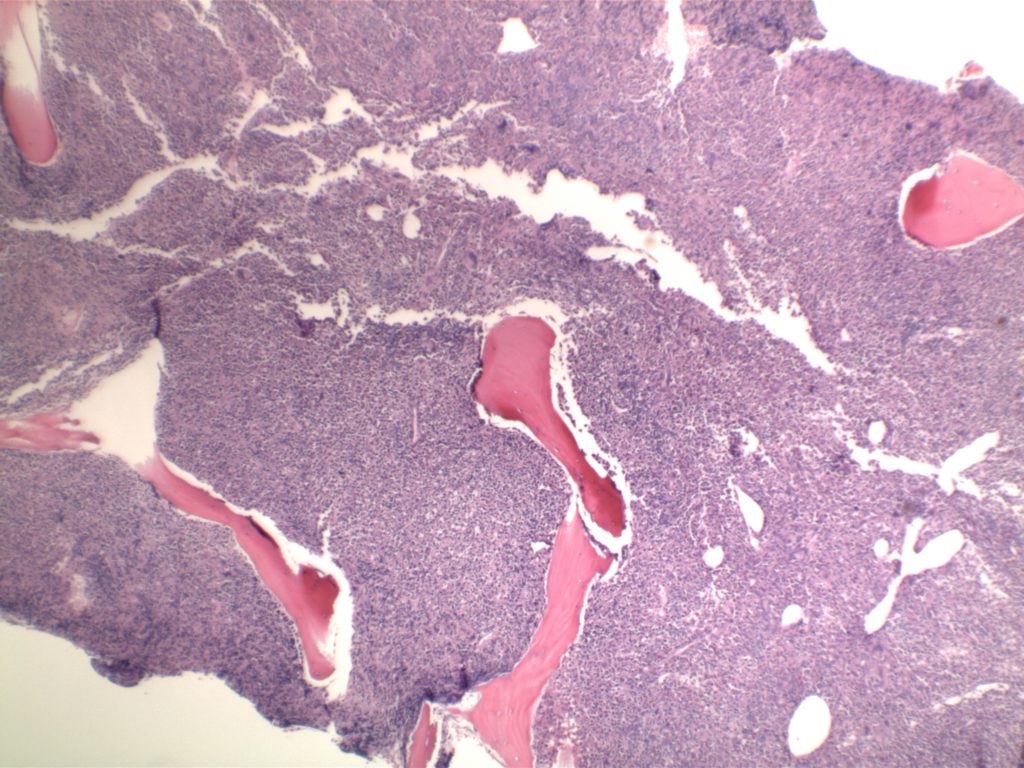
Diffuse increase of reticulin fibers with increased density and numerous intersections. Increased thick bundles of fibers consistent with collagen fibrosis. Osteosclerosis usually present.
In cases of MF2 or MF3, it is recommended to perform trichrome stain to evaluate for collagen fibrosis.
MF – Accelerated phase = 10-19% blasts in the peripheral blood and/or the bone marrow.
MF – Acute Transformation = ≥20% blasts in the blood or bone marrow.
The use of immunohistochemistry (IHC) in many of the myeloproliferative neoplasms is limited. Identifying an increased blast population is one of the most useful, and may indicate a more aggressive course or transformation to acute leukemia. Helpful IHC markers may include:
CD117 is a specific myeloid marker, and marks a subset of myeloblasts. The expression is dim, and one often must look at 20-40X to clearly see expression. Mast cells (fried egg looking cell) will have very strong expression.
CD71 marks nucleated erythroid cells. This may be helpful in quantitating and differentiating erythroid cells from myeloid cells. This marker may be set-up as a double stain with CD34.
In the setting of hematopoietic cells, E-Cadherin marks immature erythroid cells. Like CD71, E-Cadherin may be useful to differentiate immature erythroid cells from immature myeloid cells.
TdT is a sensitive lymphoblast (~95%) marker. It is not entirely specific for lymphoblasts, but other markers can help clarify diagnostic difficulties (B and T-cell markers).
References
Swerdlow SH, Campo E, Harris, NL, Jaffe ES, Pileri SA, Stein H, Thiele J (Eds): WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (Revised 4th edition). IARC: Lyon 2017
Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127: 2391–2405. doi:10.1182/blood-2016-03-643544
Kim SY, Im K, Park SN, Kwon J, Kim J-A, Lee DS. CALR, JAK2, and MPL mutation profiles in patients with four different subtypes of myeloproliferative neoplasms: primary myelofibrosis, essential thrombocythemia, polycythemia vera, and myeloproliferative neoplasm, unclassifiable. Am J Clin Pathol. 2015;143: 635–644. doi:10.1309/AJCPUAAC16LIWZMM
Tefferi A, Lasho TL, Finke CM, Knudson RA, Ketterling R, Hanson CH, et al. CALR vs JAK2 vs MPL-mutated or triple-negative myelofibrosis: clinical, cytogenetic and molecular comparisons. Leukemia. 2014;28: 1472–1477. doi:10.1038/leu.2014.3
CLL/SLL represents a B-cell neoplasm of small lymphocytes which involve a combination of peripheral blood, bone marrow, and/or lymph nodes. When peripheral blood predominates, then it is referred to as CLL, and when it presents as predominately nodal involvement it is referred to as SLL. This is the same disorder with different manifestations.
Monoclonal B-cell lymphocytosis (MBL) was defined by the International Familial CLL consortium in 2005 as a monoclonal B-cell lymphocyte population in the peripheral blood <5,000/uL without evidence of lymphadenopathy (i.e. SLL), an autoimmune/infectious disease or other features diagnostic of a B-cell lymphoproliferative disorder. The 2016 WHO hematopathology revision dropped the requirement of cytopenias or disease related symptoms as adequate to make the diagnosis of CLL.