
Mammaglobin is an antibody that marks breast duct-lobular epitheliam, salivary gland epithelium, & skin eccrine epithelium. In neoplastic tissue is may stain cases of breast carcinoma, salivary gland tumors, endocervical CIS, and endometiral carcinoma. GCDFP-15 performs a little better than mammaglobin, and may have a better specificity profile.
Category Archives: Breast
Breast Myofibroblastoma
Myofibroblastoma (MFB) of the breast is an uncommon but well described benign stromal neoplasm of the breast. MFB can have many different morphologic patterns (see variants below), but important defining characteristics include:
- Mesenchymal tumor without epimyoepithelial elements
- No necrosis
- Low proliferative activity (≤2 mitoses/10 hpf)
- No atypical mitoses
- Characteristic immunophenotype
Special Subtypes of Breast Carcinoma
-
Lobular Carcinoma
-
Medullary Carcinoma
- Pattern characteristic of BRCA1 associated carcinomas
- 13% are medullary type
- 60% have subset of medullary features
- Well-circumscribed mass
- Solid sheets of pleomorphic large cells containing prominent nucleoli In >75% of the mass
- Frequent mitosis
- Prominent lymphoplasmacytic inflammatory infiltrate surrounding and infiltrating the tumor
- Pushing/non-infiltrating border
- DCIS is minimal or absent
- WHO recommends classifying tumor as “carcinomas with medullary features”
- Pattern characteristic of BRCA1 associated carcinomas
-
Micropapillary Carcinoma
-
Mucinous (colloid) carcinoma
-
Tubular Carcinoma
-
Papillary Carcinoma
-
Secretory Carcinoma
-
Inflammatory Carcinoma
- Clinically present with breast erythema and thickening (peau d’orange)
- Dermal lymphatics filled with tumor
- 3-year survival rate 3-10%
-
Neuroendocrine Tumors
- Well-differentiated Neuroendocrine Tumor
- Small Cell Carcinoma
References
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015.
Breast – Tubular Carcinoma
Mucinous (Colloid) Carcinoma
General
- Well-circumscribed
- Neoplastic cells within lakes of mucin
Invasive Lobular Carcinoma
General
- Loss of E-Cadherin (CDH1 gene) expression
- Minimal desmoplasia and can be difficult to identify grossly (clear margins may be difficult to achieve)
- Single file infiltrating cells
Breast – Invasive Carcinoma
Invasive Breast Carcinoma
- Invasive breast carcinomas not segregated out as a special subtype are classified as invasive ductal carcinoma, no special type (NST). These tumors (and most of the special types) have prognosis and treatment plans based on the receptor status (and sometimes additional molecular profiling).
- Receptor testing includes ER/PR/Her-2 and Ki-67 (proliferation marker)
Breast Carcinoma – Risk Factors
- Most common cancer in women (~225,000 cases/yr. with ~40,000 deaths/yr.)
- Second most common cause of cancer death in women (lung #1)
- Three major subtypes
- ER+/Her-2 negative (50-65%)
- Her-2 + (10-20%)
- Triple negative – ER/PR/Her-2 negative (10-20%)
- Breast cancers in African American women are more aggressive biologically, and are more likely to be ER-negative and high nuclear grade
Breast Carcinoma – Genetic Characteristics
Approximately 12% of breast cancers are due to inheritable mutations (most common BRCA1, BRCA2, TP53, and CHEK2) Continue reading Breast Carcinoma – Genetic Characteristics
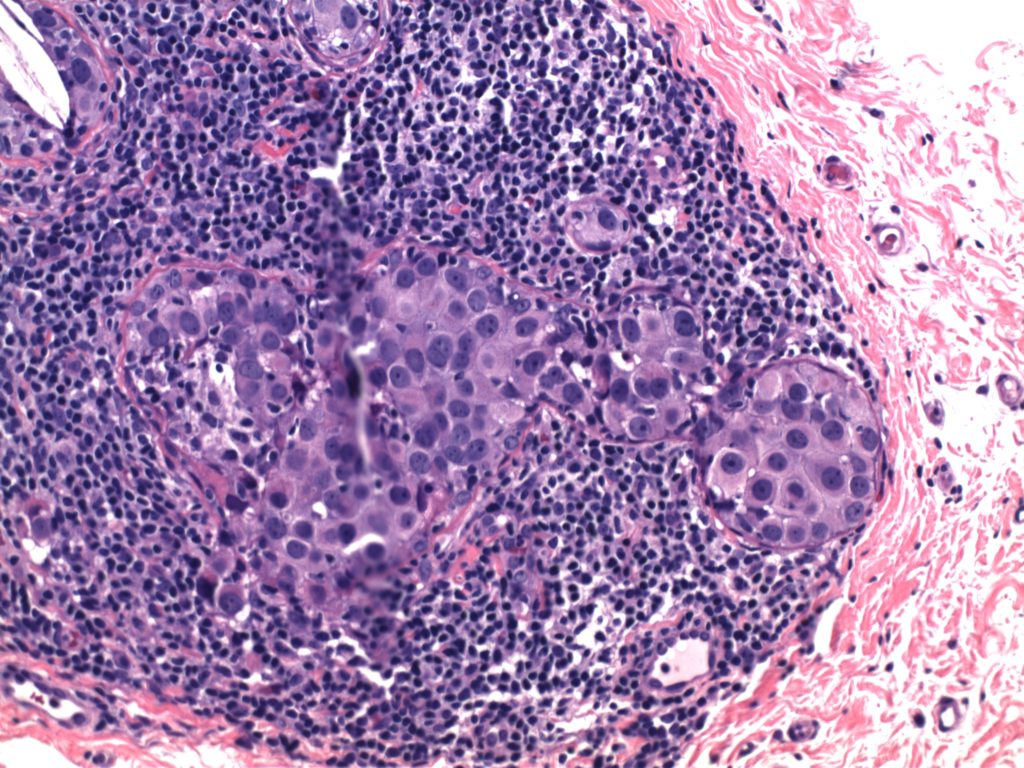
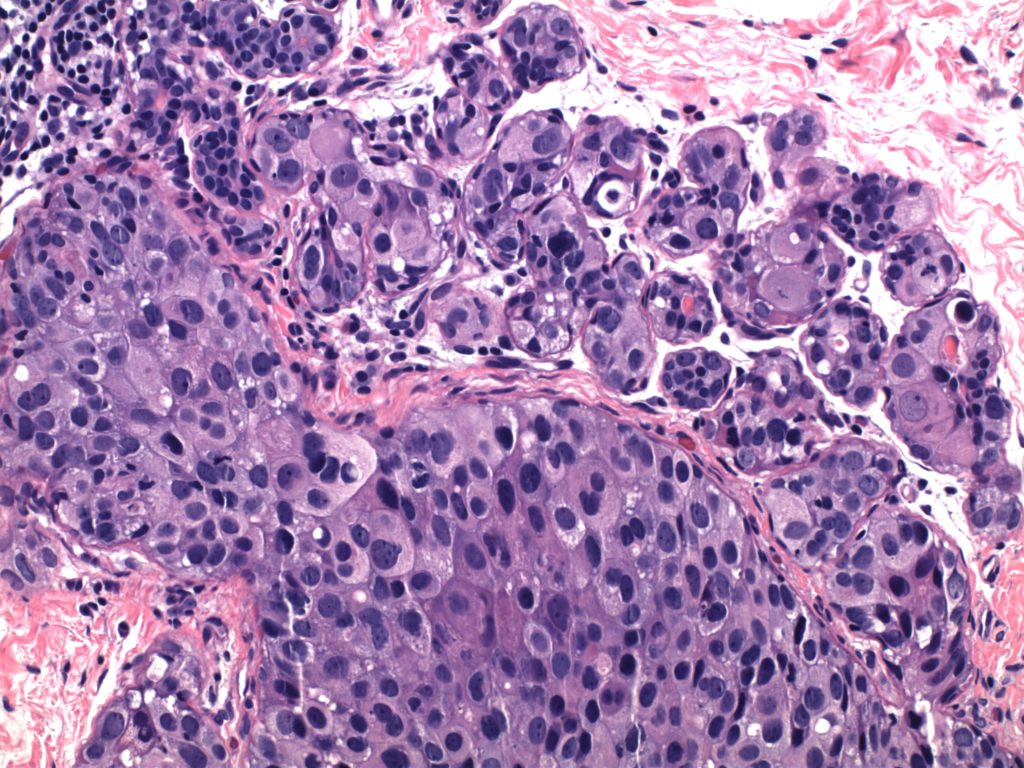
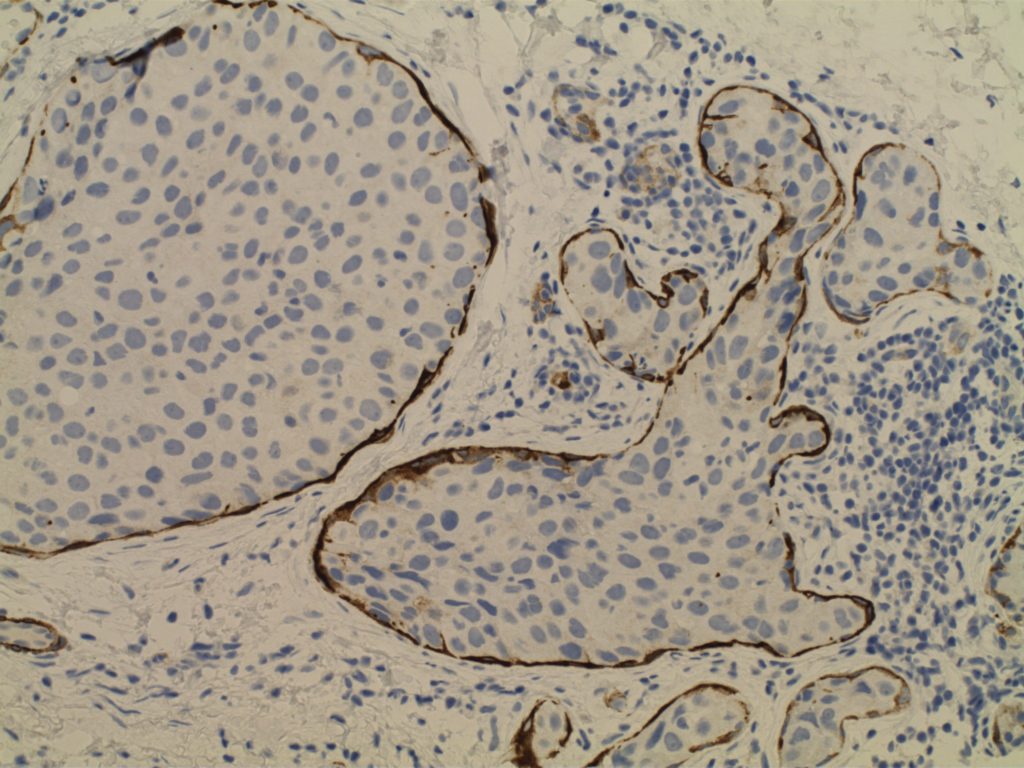
Breast – DCIS
Ductal Carcinoma In Situ (DCIS)
- Neoplastic proliferation resembling small ducts with expanded duct and acinar structures
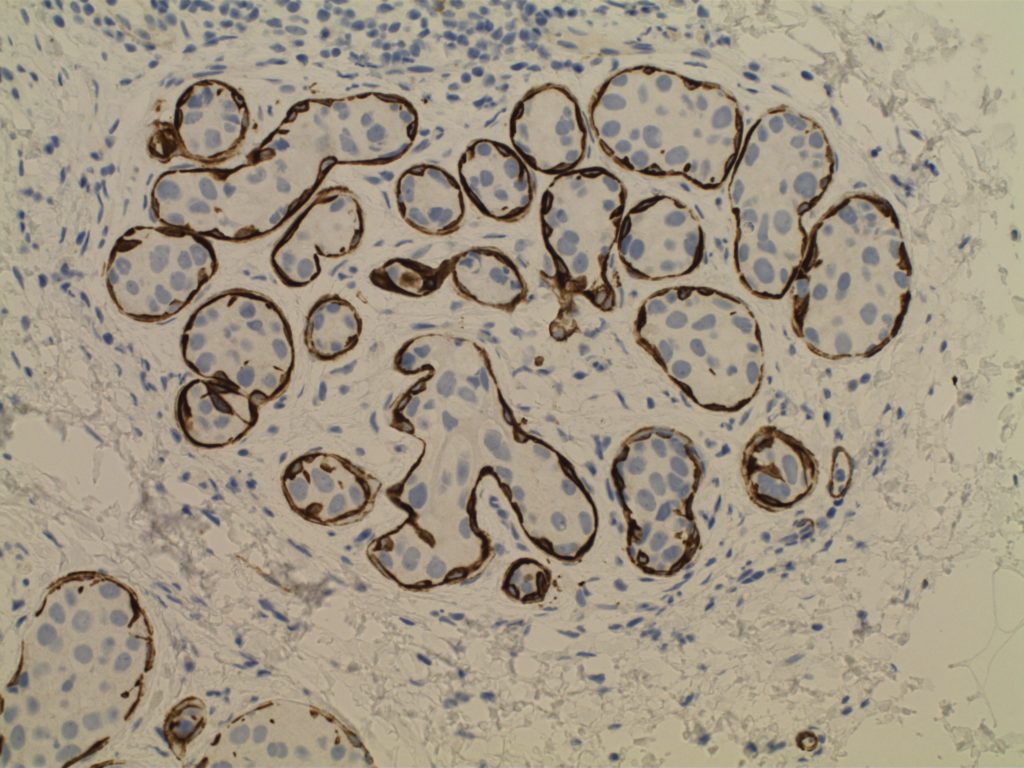
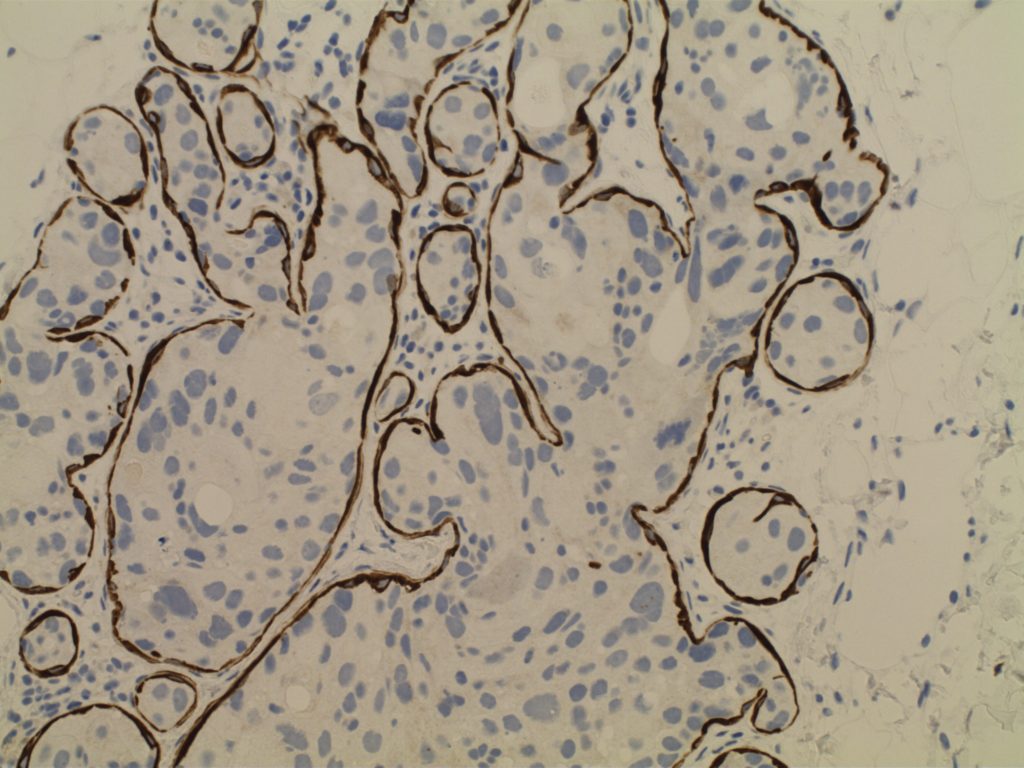
- Myoepithelial cell layer is intact surrounding the neoplastic proliferation (non-invasive tumor)
- Typically express E-Cadherin
- Bilateral in 10-20% of cases
- Detected by mammography (not clinically evident)
- Represents 15-30% of neoplasms identified in screening populations
- Typically identified by abnormal calcification, sometimes as abnormal densities
Comedo DCIS
- High grade pleomorphic nuclei
- Central necrosis
Non-comedo DCIS
- Lacks either high grade nuclei or central necrosis
- Subtypes/patterns
- Solid DCIS
- Micropapillary DCIS
- Cribiform DCIS
- DCIS grading
- Low-grade DCIS
- 1%/year risk of developing an invasive carcinoma
- Intermediate-grade DCIS
- High-grade DCIS
- Low-grade DCIS
Paget Disease
- Nipple manifestation of disease (1-4% of cases) – looks like eczema on the nipple
- Tumor cells extend into the epidermis of the skin overlying the nipple from underlying DCIS within the ductal system of the breast.
- 50-60% of women will have an underlying palpable mass
- Vast majority will have an invasive carcinoma (often ER neg./Her-2 pos.)
- Women without a palpable mass will usually only have DCIS
Photomicrographs
References
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015.