The Bloom-Richardson grading system was refined in the Nottingham/Tenovus Primary Breast Cancer Study (1974) into what is now referred to as the Nottingham grading system. This is a semi-quantitative evaluation with better inter-observer reproducibility and evaluation criteria.
For many years it was noted that tumor differentiation corresponded to prognosis. Bloom and Richardson in 1957 published the first widely known study, which showed that taking into account nuclear atypia, tubule formation, and mitotic activity of the tumor could result in a numeric grading system.
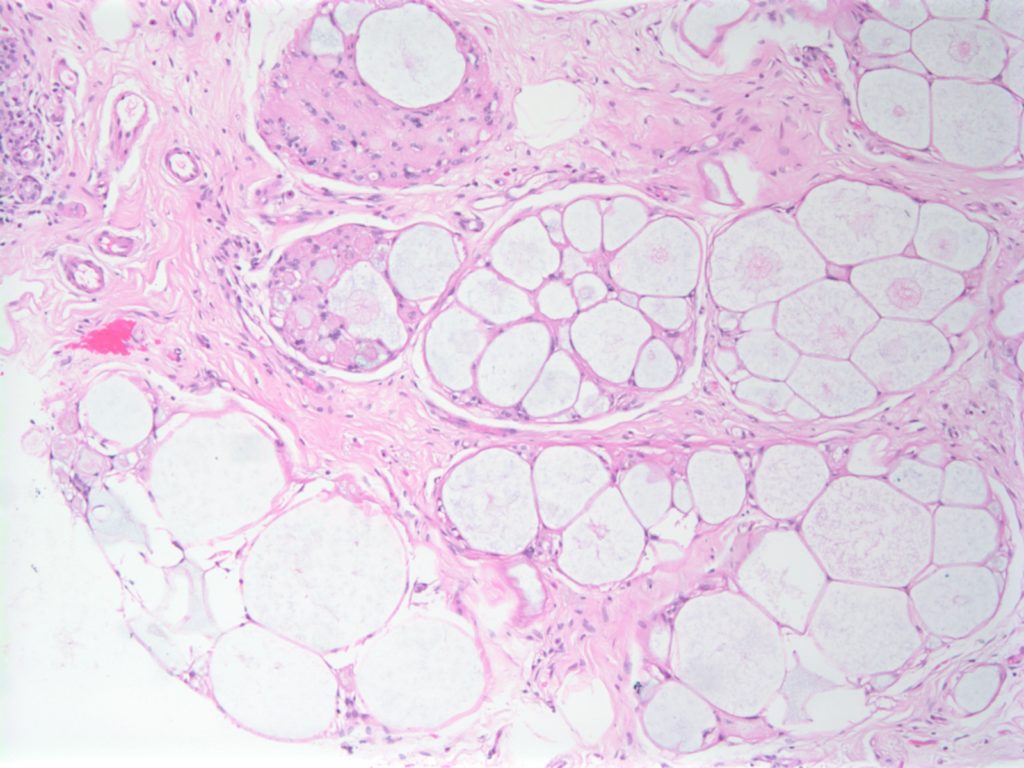
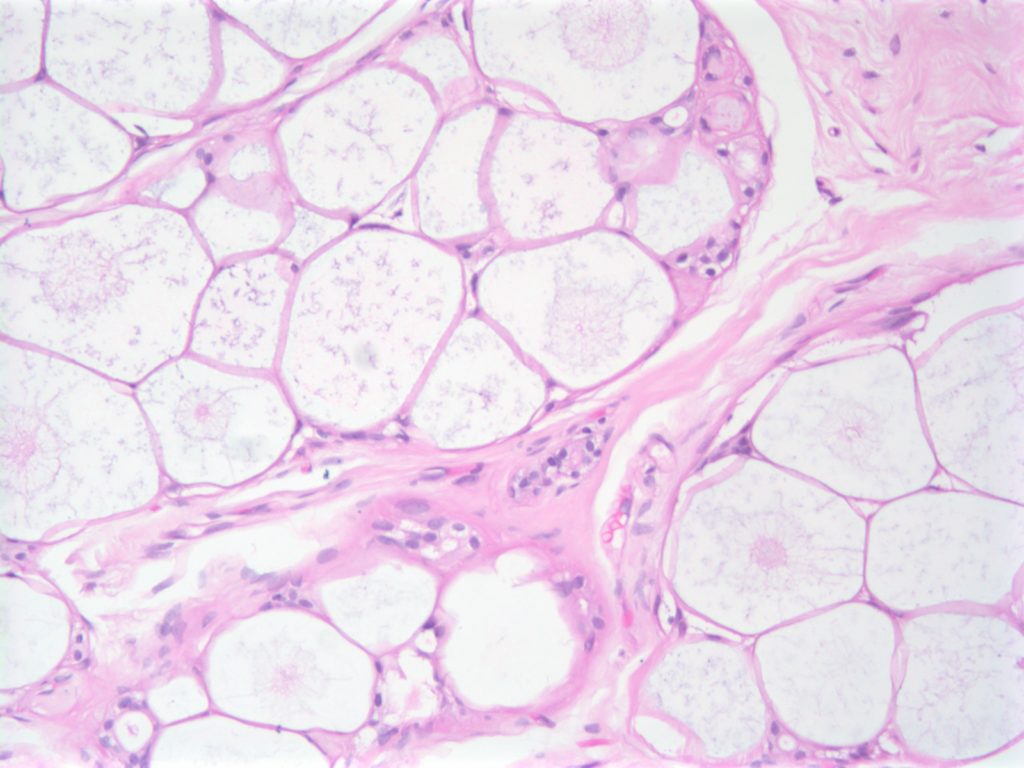
Collagenous Spherulosis is an uncommon incidental benign finding, which can be confused with other pathologies such as DCIS, carcinoma, and adenoid cystic carcinoma of the breast.
The lesions are characterized by central mucin with epithelial cells (luminal and myoepithelial) radially arranged at the periphery.
Photomicrographs
Breast – Collagenous SpherulosisBreast – Collagenous Spherulosis
References
Resetkova, E., et. al. “Collagenous spherulosis of breast: morphologic study of 59 cases and review of the literature.”. Am J Surg Pathol. 30 (1):207. Jan 2006. doi:10.1097/01.pas.0000179237.91515.81
Fat necrosis may sometimes present as a palpable mass, which may raise clinical concern or distress in the patient. Approximately 1/2 of cases have a history of trauma. Fat necrosis is also a common finding in excision specimen after a preceding biopsy.
The characteristic findings of fat necrosis include mixed inflammation (neutrophils, histiocytes, etc.), fibroblastic proliferation, and liquefactive fat necrosis. Each of the component may vary in prominence. The most important thing is not to mistake fat necrosis for malignancy, and not miss an area of malignancy masked by fat necrosis (AE1/AE3 or CAM5.2 may be helpful in such situations).
Photomicrographs
Fat NecrosisFat NecrosisFat Necrosis with giant cell reaction
References
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015.
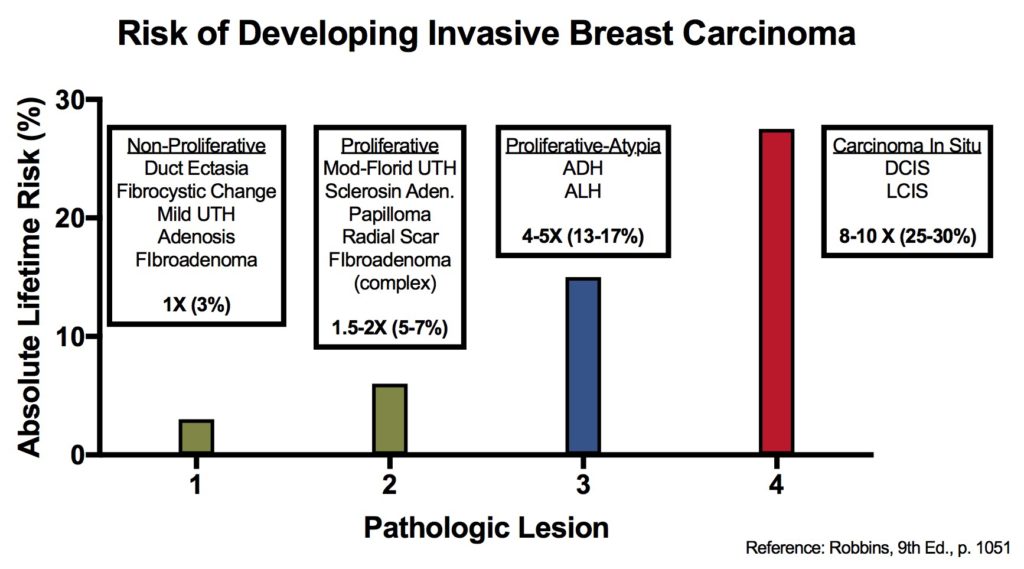
There are many features of breast disease that encompass a wide spectrum of morphologic and radiologic findings, which have a varying risk of subsequent carcinoma. Some of these entities are thought to be direct precursors to invasive carcinoma, and others just signify a component of future risk of invasive carcinoma.
There are multiple situations where immunohistochemistry can serve an important role in breast disease. These include: differentiation of lesion types (e.g. UTH vs. ADH), identifying invasion (e.g DCIS vs. DCIS with invasion), and predictive/prognostic information (e.g. ER/PR/HER-2).
The following table and figure illustrate the risk of developing an invasive breast carcinoma based on the type of lesions previously identified. This information does not take into consideration other factors such as race and family history (complicated topic).
Relative and Absolute Risk of Invasive Breast Carcinoma
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015.
Atypical lobular hyperplasia is a proliferation of epithelial cells in the terminal duct-lobular unit that lacks expression of E-cadherin and fills the lobular unit (but does not expand). Some define ALH as filling or distending <50% of the acini within an affected lobule. There is some variation between experts as the exact differentiating line between ALH and lobular carcinoma in situ (LCIS). It is best to think of ALH and LCIS as representing a morphologic spectrum with filling and distention of lobular acini being the measured characteristic.
In some cases ALH/LCIS may appear similar to DCIS or merge with areas of DCIS. E-cadherin is a helpful marker to differentiate between these lesions. Clinically it is important to differentiate ALH/LCIS from DCIS because LCIS/ALH is an incidental finding on mammogram and represents a risk factor for bilateral breast carcinomas. Management is not through local excision, but surveillance and hormonal therapy dependent upon the type of lesion. DCIS is treated through local excision because these lesions tend to be localized/focal.
ALH carries an increased risk of developing an invasive breast carcinoma (4-5x relative risk, 13-17% lifetime risk), while LCIS carries an 8-10x increased relative risk, 25-30% lifetime risk). These are the same risks as ALH and DCIS, respectively. Although ALH/LCIS risk is bilateral, while ADH/DCIS tends to be more ipsilateral.
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015. p. 1050-1051
Introductal papilloma can have varying appearances but characteristically contain an ductal epithelial proliferation on a fibrovascular core with an intact myoepithelial layer. Larger duct lesions are located near the nipple and typically produce a discharge (~80%). Small duct lesions are frequently multiple and located deeper in the breast.
Papilloma are are associated with a slight increased risk for breast carcinoma (1.5-2x increased relative risk). The absence of a myoepithelial layer is not characteristic of a typical papilloma, and likely represents a different papillary lesion.
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015. p. 1048-1051