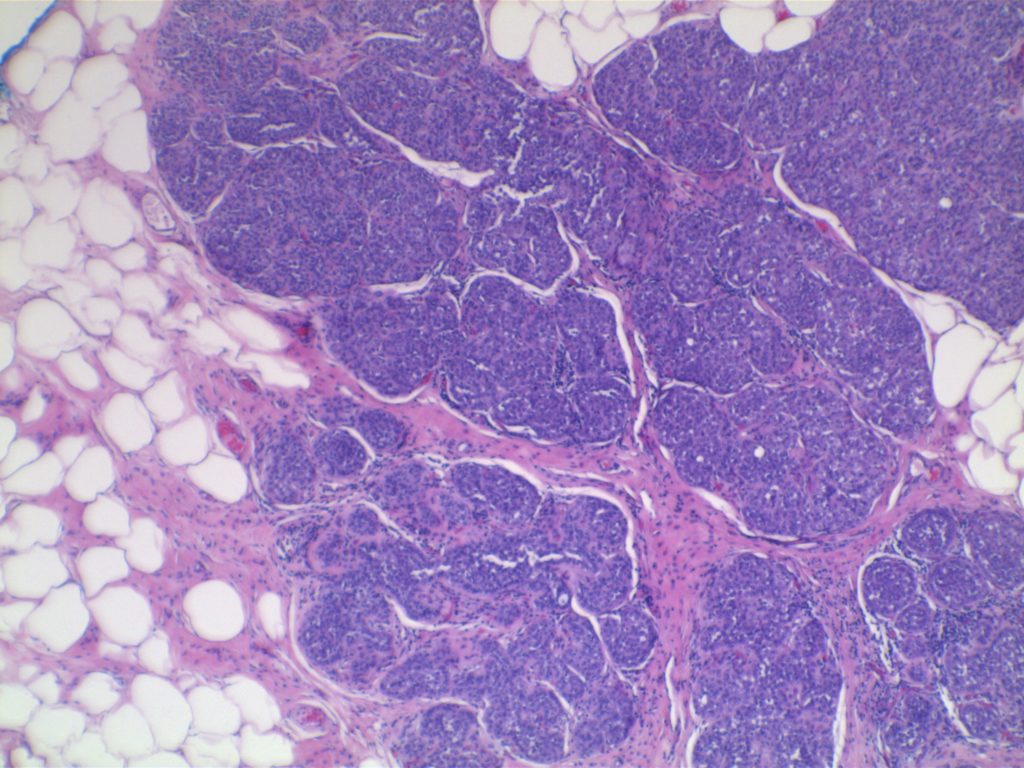
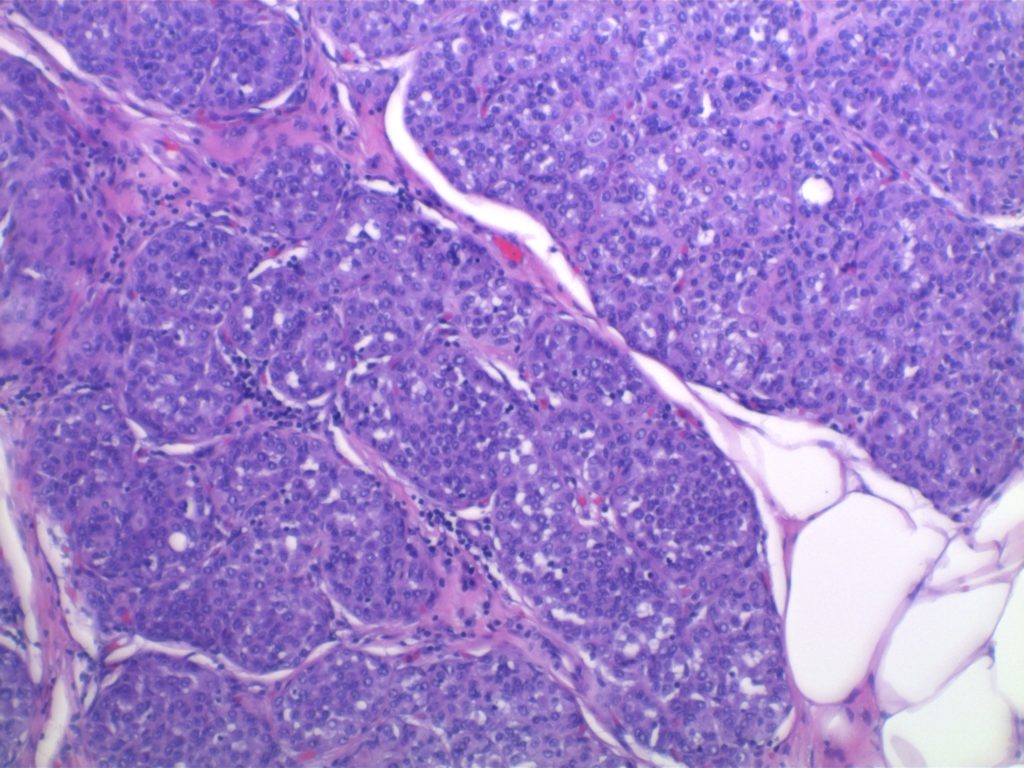
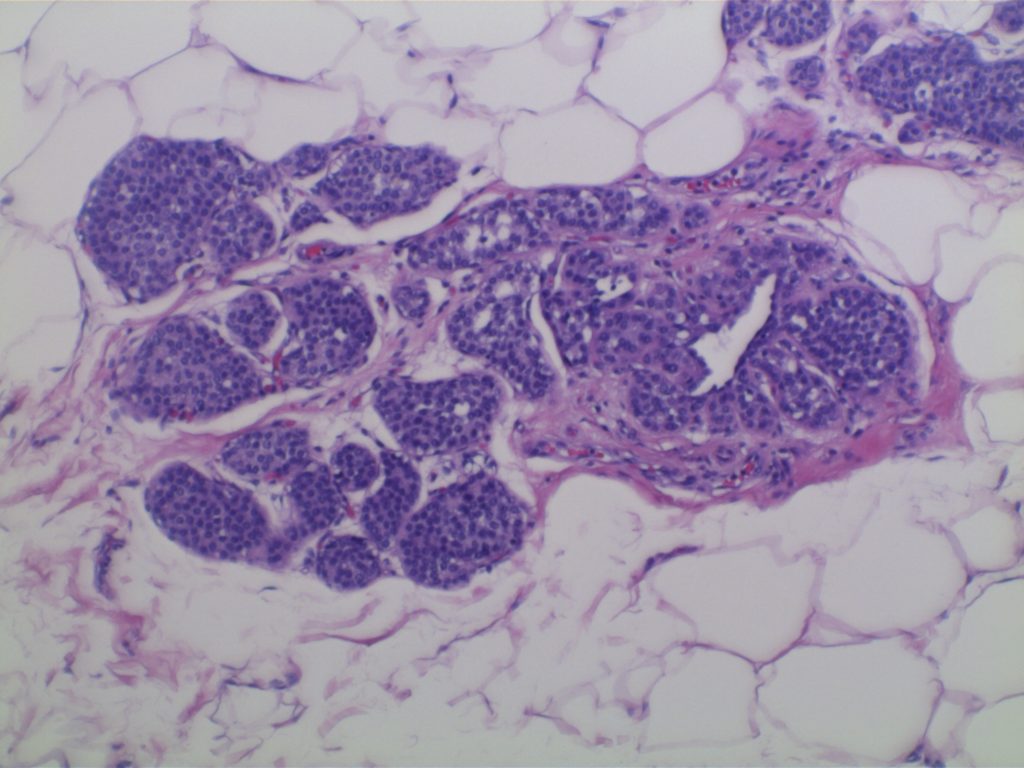
As the name indicates a complex sclerosing lesion is “complex” in that it has multiple parts, which contribute to is “scar-like” appearance. These lesions can be detected frequently by mammography mimicking invasive carcinoma, and subsequently leads to biopsy.
These lesions contain a combination of different patterns discussed elsewhere, including sclerosing adenosis, papilloma, usual type hyperplasia (UTH), and fibrosis. The architecture of this lesion is around a central area of compressed entrapped ducts within fibrosis, which radiate outward with varying dilation of duct structures and present of epithelial hyperplasia.
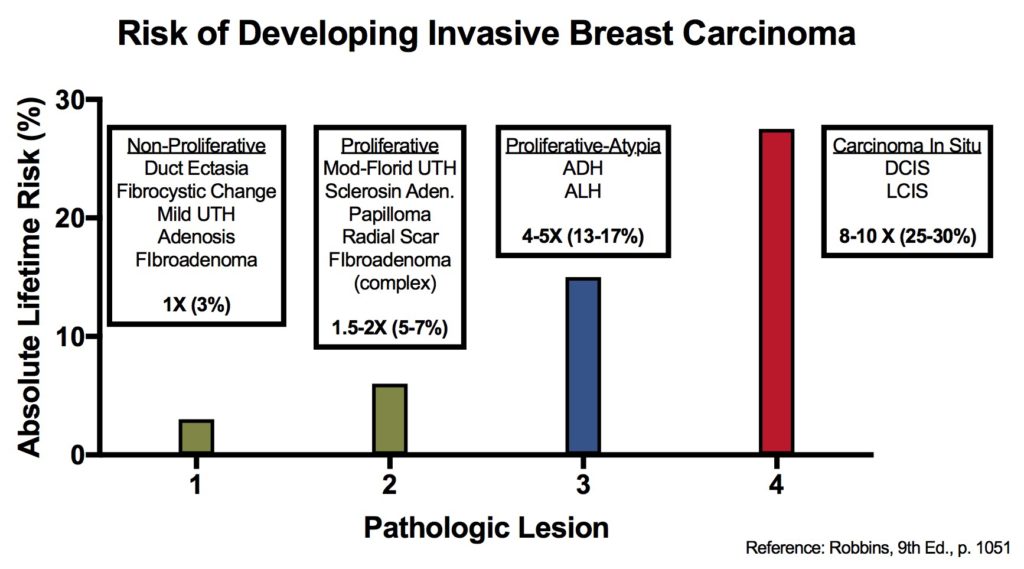
Complex scoring lesions are not neoplastic but are associated with a 1.5-2x increased relative risk for breast carcinoma.
Breast lesions and risk of developing an invasive carcinoma
References
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015.