Introductal papilloma can have varying appearances but characteristically contain an ductal epithelial proliferation on a fibrovascular core with an intact myoepithelial layer. Larger duct lesions are located near the nipple and typically produce a discharge (~80%). Small duct lesions are frequently multiple and located deeper in the breast.
Papilloma are are associated with a slight increased risk for breast carcinoma (1.5-2x increased relative risk). The absence of a myoepithelial layer is not characteristic of a typical papilloma, and likely represents a different papillary lesion.
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015. p. 1048-1051
As the name indicates a complex sclerosing lesion is “complex” in that it has multiple parts, which contribute to is “scar-like” appearance. These lesions can be detected frequently by mammography mimicking invasive carcinoma, and subsequently leads to biopsy.
These lesions contain a combination of different patterns discussed elsewhere, including sclerosing adenosis, papilloma, usual type hyperplasia (UTH), and fibrosis. The architecture of this lesion is around a central area of compressed entrapped ducts within fibrosis, which radiate outward with varying dilation of duct structures and present of epithelial hyperplasia.
Complex scoring lesions are not neoplastic but are associated with a 1.5-2x increased relative risk for breast carcinoma.
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015.
Sclerosing Adenosis (SA) is an increased density of duct-lobular acini, which characteristically are compressed in the central portion of the lesion with dense stroma/fibrosis. Sometimes these lesions can closely mimic an invasive ducatal carcinoma, immunohistochemistry is necessary to separate lesions.
SA is not a neoplastic process, but is associated with a 1.5-2X increased relative risk for breast carcinoma.
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015.
Non-neoplastic luminal proliferation of ductal epithelial and myoepithelial cells, which can fill and expand ductal strucutures. The morphology shows a mixed cellularity pattern with overlapping nuclei, which often have a “streaming” appearance. In challenging cases immunohistochemistry can help differentiated these lesions from ADH or DCIS.
If present only focally, there is not an increased risk of breast carcinoma. However, moderate to florid usual type hyperplasia is associated with a 1.5-2X increased relative risk of breast carcinoma.
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015.
This is a non-proliferative lesion characterized clinically as small lumps, which do not carry an increased risk of breast carcinoma. Fibrocystic changes have three characteristic features, which may be present in part or whole, and include:
Cystic change – Cysts (typically of varying sizes) lines by flat atrophic epithelium or apocrine metasplasia are characteristic. Calcification are also common.
FIbrosis – Areas of fibrosis are characteristically present, and are thought to originate from chronic inflammation secondary to ruptured cysts.
Dilated duct structures with apocrine changes (low power).Fibrocystic change with apocrine metaplasia and micropapillary formation.Duct dilation in fibrocystic change (low power).
References
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015.
HER-2 FISH amplified tumors may have 1+ (negative) or 2+ (equivocal) staining by IHC, and it is recommended that IHC and FISH be used in cases with micropapillary pattern.
Flat epithelial atypia (FEA) probably represents one of the earliest morphologically detectible findings towards the development of low-grade in situ and invasive carcinomas and lobular neoplasia. Molecular studies have shown recurrent loss of 16q, which is characteristic of low grade lesions, and gene expression profiles similar to low-grade in situ and invasive carcinomas. In the past there have been many other terms used to characterize a heterogeneous spectrum of lesions that fall under the umbrella of FEA: “small ecstatic ducts lined by atypical ductal cells with apocrine snouts,” “clinging in situ duct carcinoma flat type,” atypical cystic duct,” “DIN 1-flat type,” and “columnar alteration with prominent apical snouts and secretions with atypia.” The important take home point is that there must be low-grade atypia present to fall within this category. No atypia, then it will be described in another way (e.g. columnar cell change). If the atypic is “high-grade,” then the diagnosis of DCIS (clinging carcinoma) is warranted.
Incidental finding (not associated with calcifications or stromal reactions found by mammography)
LCIS is bilateral 20-40% of cases
Morphology
Mucin-positive signet ring cells often present
E-Cadherin negative cells
Uniform cells with oval/round nuclei
Pagetoid spread (cells present between the myoepithelial layer and over lying luminal epithelium
Typically ER/PR positive
Her-2 is not overexpressed
1%/year risk of developing an invasive tumor (similar to low-grade DCIS) – Lifetime risk is ~25-35% (20-30 year time period)
Cancer risk is equal in contralateral breast (unlike DCIS)
Pleomorphic variant of LCIS
High grade nuclei
May be ER negative
Some may overexpress Her-2
May be separate entity from typical LCIS
Photomicrographs
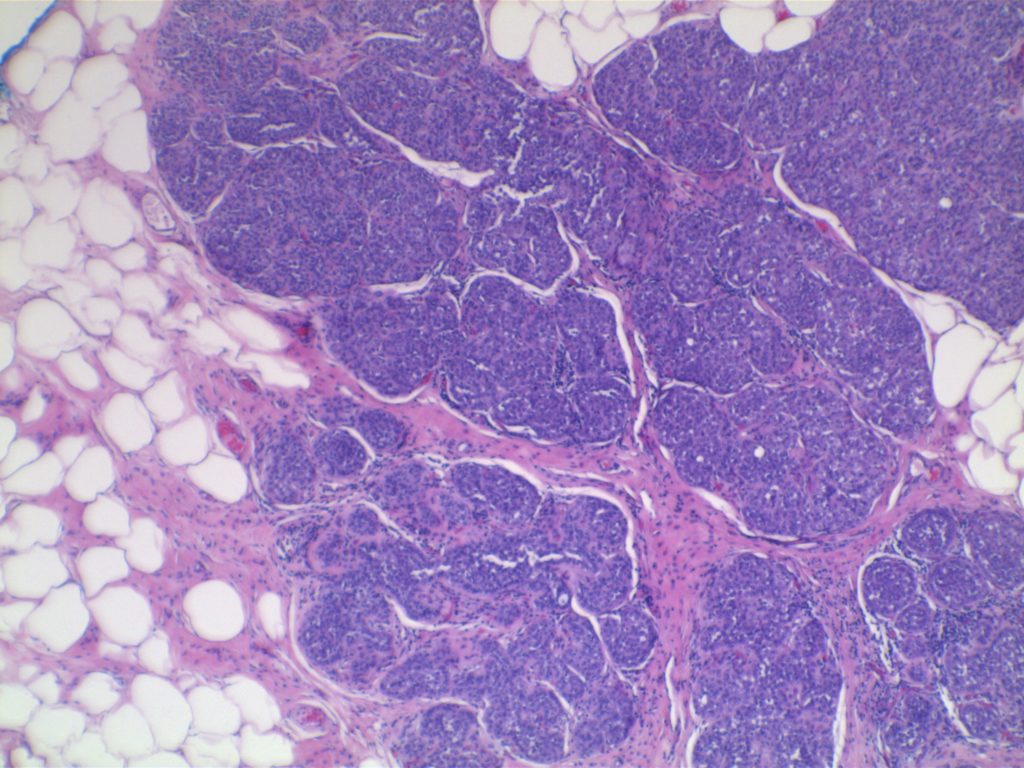
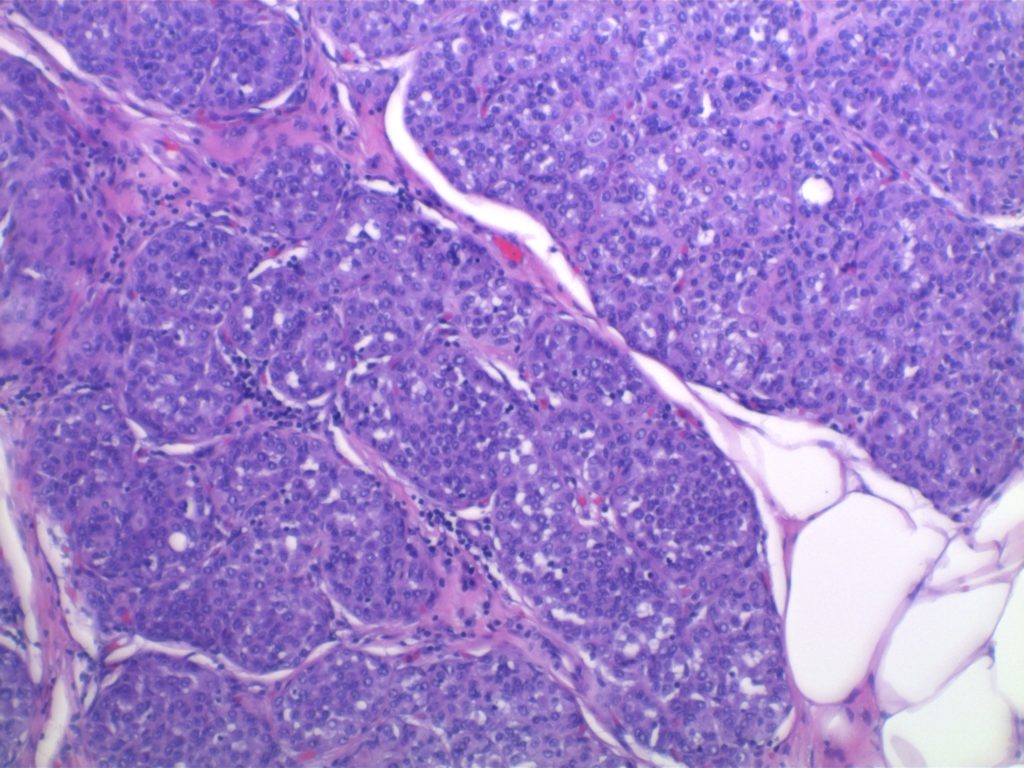
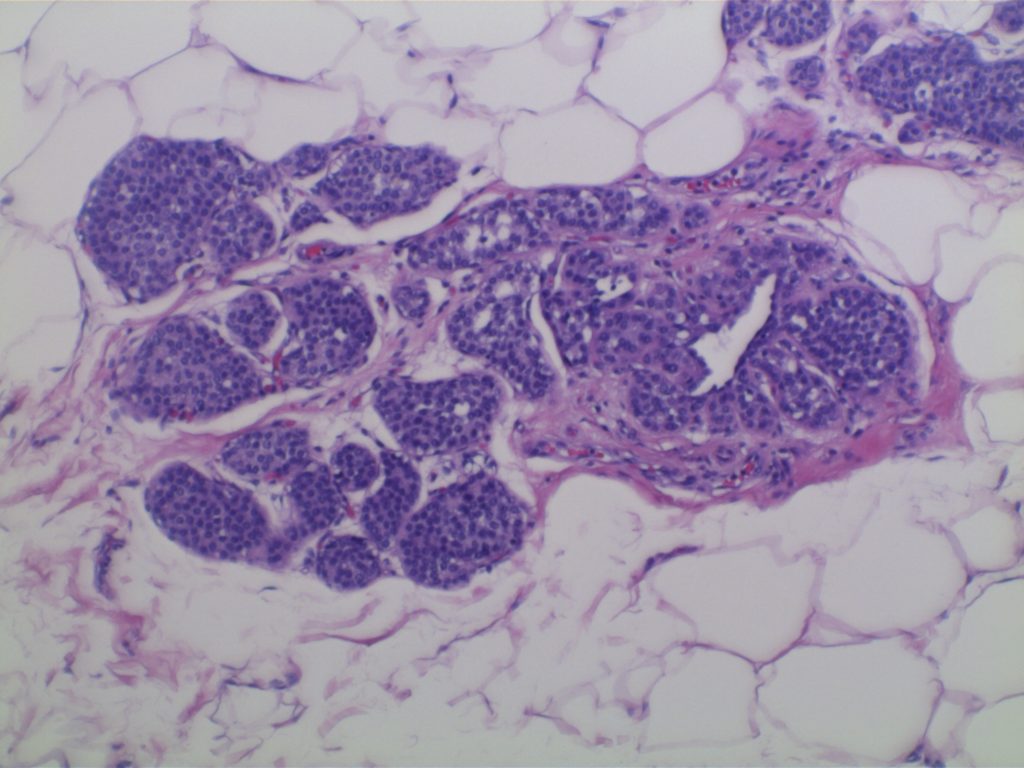
LCIS characterized by filling and expansion of the lobular unit.
LCIS characterized by filling and expansion of the lobular unit.LCIS characterized by filling and expansion of the lobular unit.
References
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015. p. 1045.
Most patients with breast symptoms present with pain, nipple discharge, palpable mass, or “lumpiness”. However, presentation of breast cancers most commonly present with an abnormal mammogram followed by a palpable mass, and as pain or nipple discharge and a small percentage of patients. For a mass to be palpable, it has to be approximately 2–3 cm in size. Mammography can detect smaller non palpable lesions at about one half of the size of palpable masses (1 cm). Mammography identifies abnormalities is either densities or calcifications. (Robbins, page 1045–1 046).
Breast symptoms
Pain
Common symptom which is often cyclic with menses
Localized pain more commonly associated with trauma, ruptured cyst, infection or idiopathic
Pain is the presenting symptom in 10% of breast cancers
Nipple discharge
Large duct papilloma-bloody/serous discharge
Milky discharge–elevated prolactin, hypothyroidism, drug effect
Malignancy risk
7%, women < 60 y/o
30%, women >60 y/o
Palpable mass
Lesions must be 2–3 cm to be clinically palpable
Most palpable lesions are benign, but finding is not specific
Malignancy risk
10%, women < 40 y/o
60%, women > 50 y/o
Location distribution of breast carcinomas
Upper outer quadrant – 50%
Central / subareolar region – 20%
Remaining quadrants – 10%
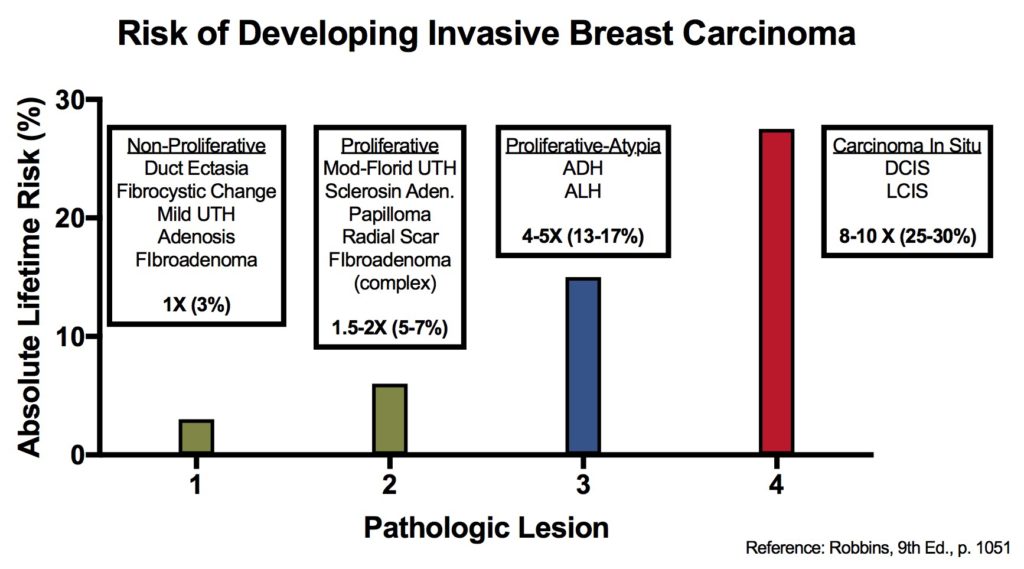
Breast lesions and risk of developing an invasive carcinoma
Kumar, Vinay, Abul K. Abbas, and Jon C. Aster. Robbins and Cotran Pathologic Basis of Disease. Ninth edition. Philadelphia, PA: Elsevier/Saunders, 2015.
Diffuse Large B-Cell Lymphoma represents a heterogeneous group of non-Hodgkin B-cell lymphoma cases that share a common architectural pattern and large cell size. Subcategorization have been attempted with varying success based on morphology, immunophenotype, and molecular characteristics. Gene expression profiling (GEP) has demonstrated two important groups for both prognosis and treatment. Alizadeh, et al showed significant survival differences in cases of DLBCL with either a germinal center B-cell-like pattern or an activated B-cell-like pattern.
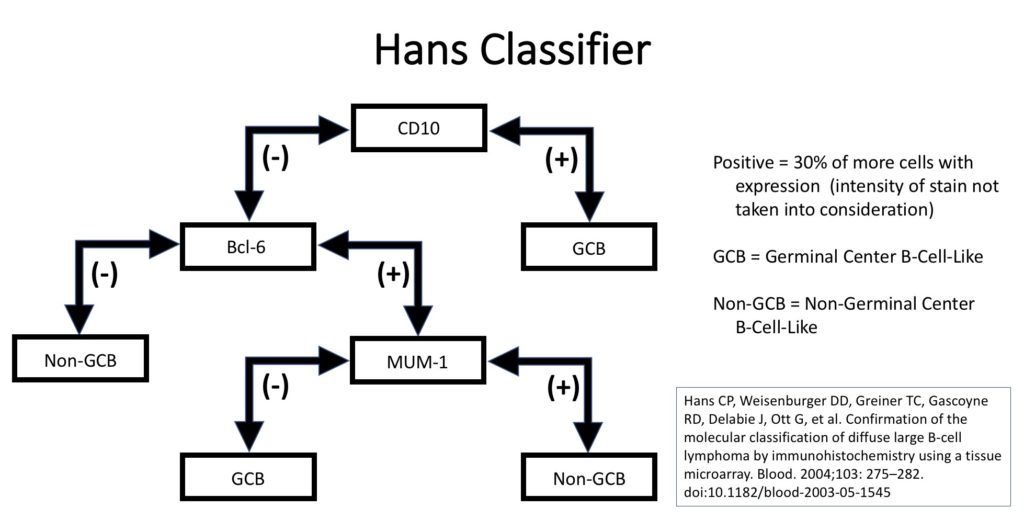
Unfortunately, GEP is not available in routine clinical practice, and multiple surrogate immunohistochemistry (IHC) based algorithms have been developed as a surrogate to GEP. The Hans’ algorithm (classifier) has been one of the most popular methods because it uses only three IHC markers (CD10, Bcl-6, & MUM-1) that are commonly available in most pathology laboratories. The following figure highlights the algorithm for the Hans’ classifier as described in the original paper. The Hans’ algorithm appears to match GEP in 75-80% of cases.
Hans classifier to subtype DLBCL as to germinal center B-cell-like (GCB) or non-germinal center B-cell-like (non-GCB) which has prognostic significance.
Alternative Algorithm(s)
The University of Nebraska group that originally developed the Hans algorithm has developed a new IHC stain algorithm that reportedly classifies cases of DLBCL more accurately compared to the corresponding molecular subtypes (~80% concordance). This algorithm uses GCET1, CD10, BCL-6, MUM-1, and FOXP1 with differing cutoff values for positive/negative. (WW Choi, et al) New algorithms with IHC markers not commonly used in many laboratories has probably limited popularity compared to the Hans’ algorithm. The 2016 WHO hematopathology revision requires that cases of DLBCL be characterized at GCB vs. non-GCB by some acceptable methodology (molecular or IHC).
References
Hans CP, Weisenburger DD, Greiner TC, Gascoyne RD, Delabie J, Ott G, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood. 2004;103: 275–282. doi:10.1182/blood-2003-05-1545
Haarer CF, Roberts RA, Frutiger YM, Grogan TM, Rimsza LM. Immunohistochemical classification of de novo, transformed, and relapsed diffuse large B-cell lymphoma into germinal center B-cell and nongerminal center B-cell subtypes correlates with gene expression profile and patient survival. Arch Pathol Lab Med. 2006;130: 1819–1824.
Chang C-C, McClintock S, Cleveland RP, Trzpuc T, Vesole DH, Logan B, et al. Immunohistochemical expression patterns of germinal center and activation B-cell markers correlate with prognosis in diffuse large B-cell lymphoma. Am J Surg Pathol. 2004;28: 464–470.
Choi WWL, Weisenburger DD, Greiner TC, Piris MA, Banham AH, Delabie J, et al. A new immunostain algorithm classifies diffuse large B-cell lymphoma into molecular subtypes with high accuracy. Clin Cancer Res. 2009;15: 5494–5502. doi:10.1158/1078-0432.CCR-09-0113
Alizadeh AA, Elsen MB, Davis RE, Ma C. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. 2000.
Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127: 2375–2390. doi:10.1182/blood-2016-01-643569