
Major Criteria
- Platelet count ≥450,000/μL
- Presence of JAK2, CALR, or MPL mutation
- Does not meet the WHO criteria for another myeloid neoplasm
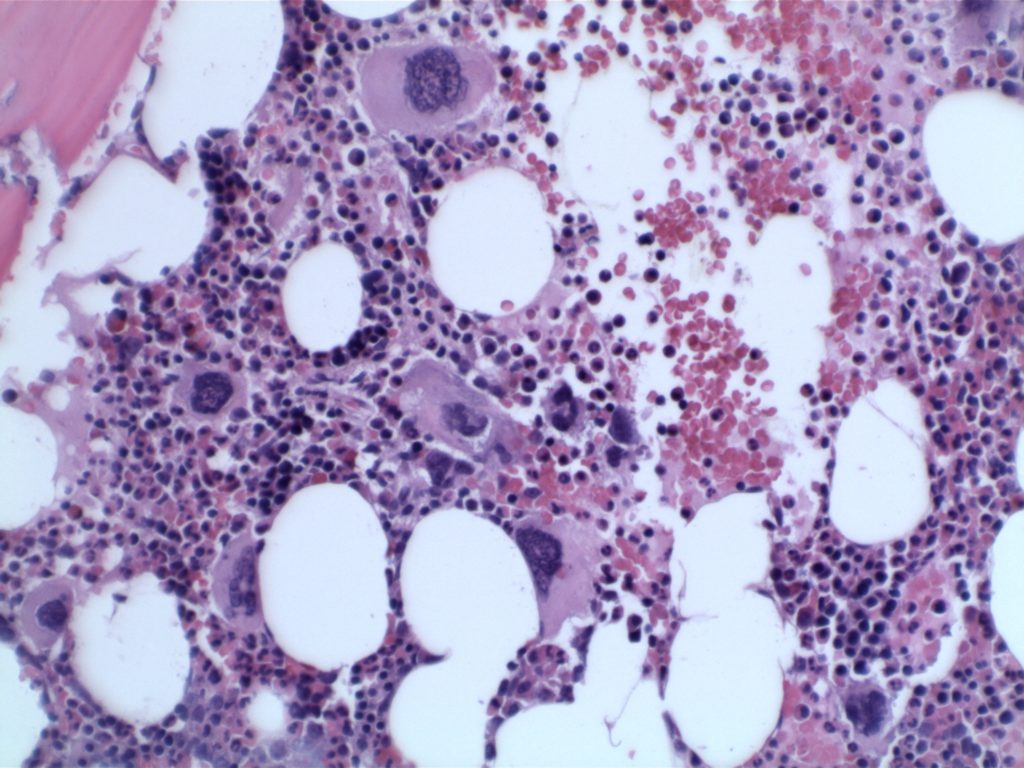
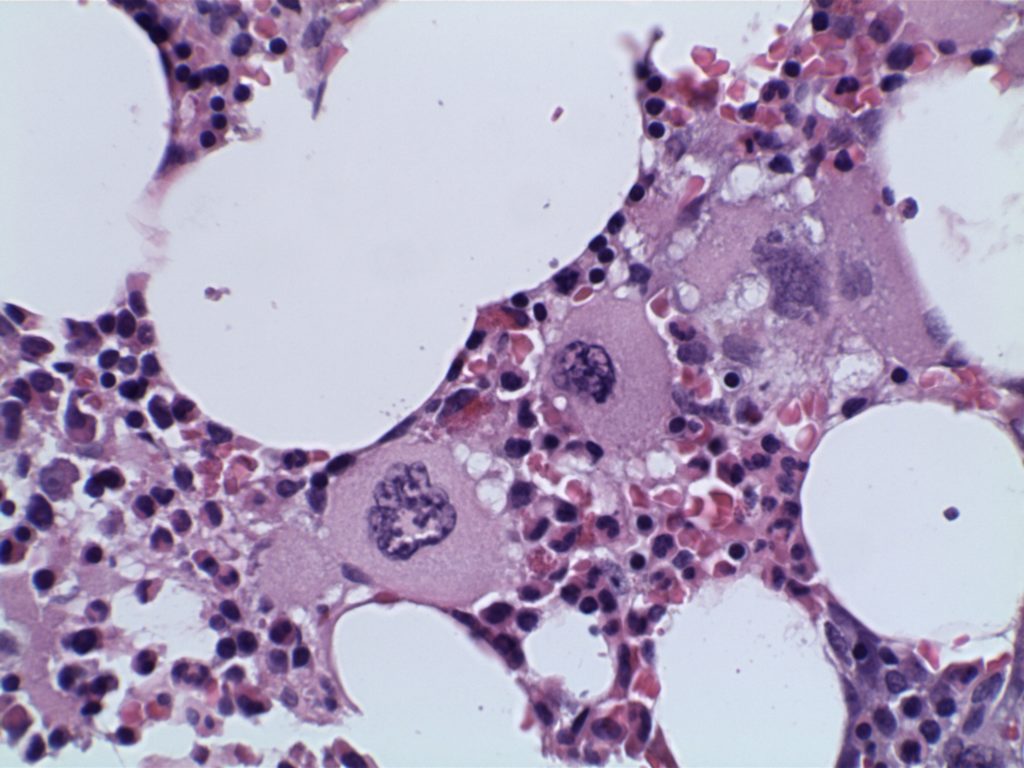
- BM biopsy showing megakaryocytic proliferation
- Enlarged mature megakaryocytes
- Hyperlobated nuclei (not as pleomorphic or bizzare as in PMF)
- Granulopoiesis and erythropoiesis is not increased or left shifted
- No more than MF1 reticulin fibrosis
Minor Criteria
- Evidence of a clonal marker or exclusion of reactive thrombocytosis
Diagnosis of ET is confirmed by all four major criteria, or if there is no evidence of a JAK2, CALR, or MPL mutation (major criterion #2), then the presence of the minor criterion.
Frequency of Molecular Abnormalities
- JAK2 – 63% (V617F mutation)
- CALR – 18%
- MPL – 2-3%
Overall, approximately 83% of cases of ET have either a JAK2, CALR, or MPL mutation (n=79).
Photomicrographs
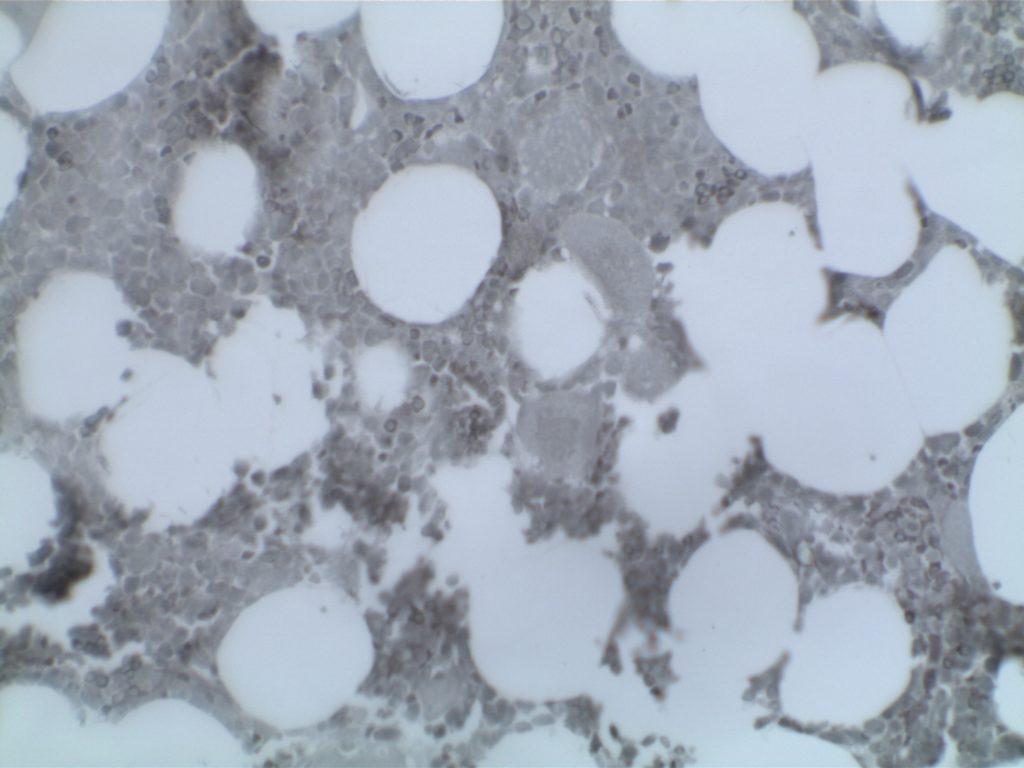
Immunohistochemistry
The use of immunohistochemistry (IHC) in many of the myeloproliferative neoplasms is limited. Identifying an increased blast population is one of the most useful, and may indicate a more aggressive course or transformation to acute leukemia. Helpful IHC markers may include:
|
Stain
|
Comment
|
|
CD34 marks immature cells including myeloblasts. In the setting of AML, it is ~70% sensitive. A subset of lymphoblasts may express CD34.
|
|
|
CD117 is a specific myeloid marker, and marks a subset of myeloblasts. The expression is dim, and one often must look at 20-40X to clearly see expression. Mast cells (fried egg looking cell) will have very strong expression.
|
|
|
CD71 marks nucleated erythroid cells. This may be helpful in quantitating and differentiating erythroid cells from myeloid cells. This marker may be set-up as a double stain with CD34.
|
|
|
In the setting of hematopoietic cells, E-Cadherin marks immature erythroid cells. Like CD71, E-Cadherin may be useful to differentiate immature erythroid cells from immature myeloid cells.
|
|
|
TdT is a sensitive lymphoblast (~95%) marker. It is not entirely specific for lymphoblasts, but other markers can help clarify diagnostic difficulties (B and T-cell markers).
|
References
Hematopathology. [edited by] Jaffe, ES. 1st. ed. Elsevier, Inc. © 2011.
Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127: 2391–2405. doi:10.1182/blood-2016-03-643544
Kim SY, Im K, Park SN, Kwon J, Kim J-A, Lee DS. CALR, JAK2, and MPL mutation profiles in patients with four different subtypes of myeloproliferative neoplasms: primary myelofibrosis, essential thrombocythemia, polycythemia vera, and myeloproliferative neoplasm, unclassifiable. Am J Clin Pathol. 2015;143: 635–644. doi:10.1309/AJCPUAAC16LIWZMM