DLBCL associated with chronic inflammation is a special subtype of DLBCL first described in 1987 and subsequently recognized as a specific and separate entity in the 2008 WHO hematopathology classification.
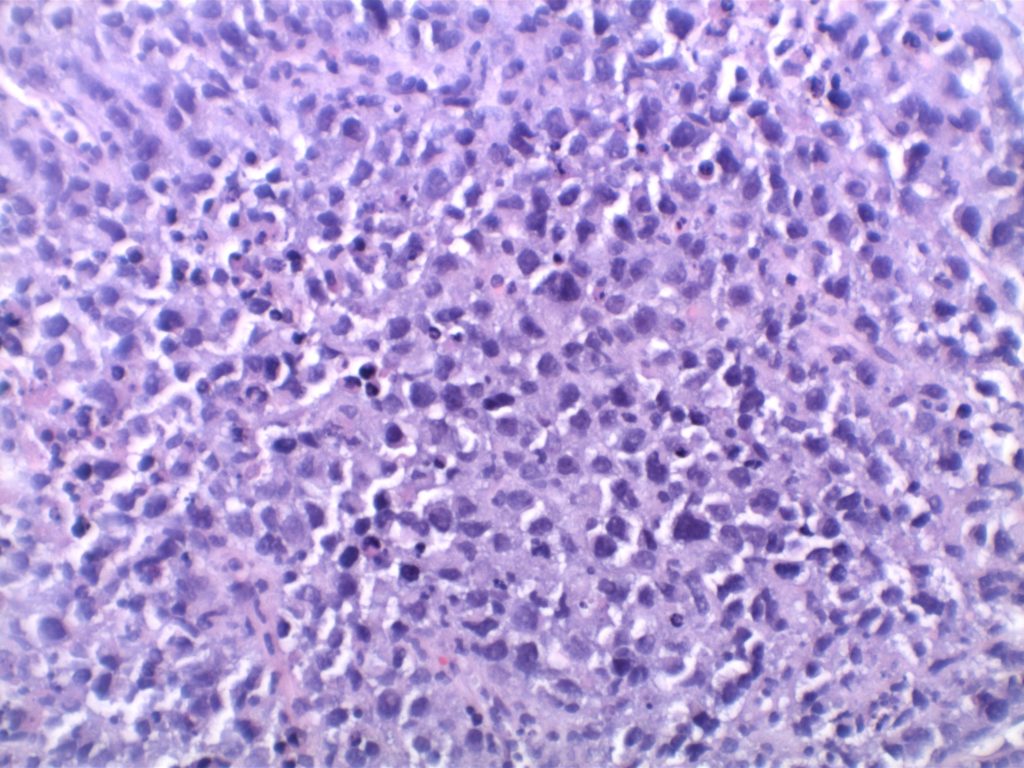
Morphologically, it is recognized as a diffuse large B-cell lymphoma that arises in the setting of long-standing chronic inflammation and is associated with EBV infection. Commonly, these present as tumor masses involving body cavities. This is classically and originally described as pleural-based lesions in patients with chronic pyothorax (artificial pneumothorax for pulmonary tuberculosis or tuberculosis pleuritis).
Originally, these were designated as ‘pyothorax-associated lymphomas’ (PAL) and characteristically are associated with EBV. It is thought that these lesions arise as a result of ‘local’ immunodeficiency, and seem to carry the following common characteristics (regardless of location):
Association with EBV
Confined space (often body cavity)
Long standing/slow growing lesion associated with chronic inflammation
Morphologic characteristics of diffuse large B-cell lymphoma
Immunophenotype
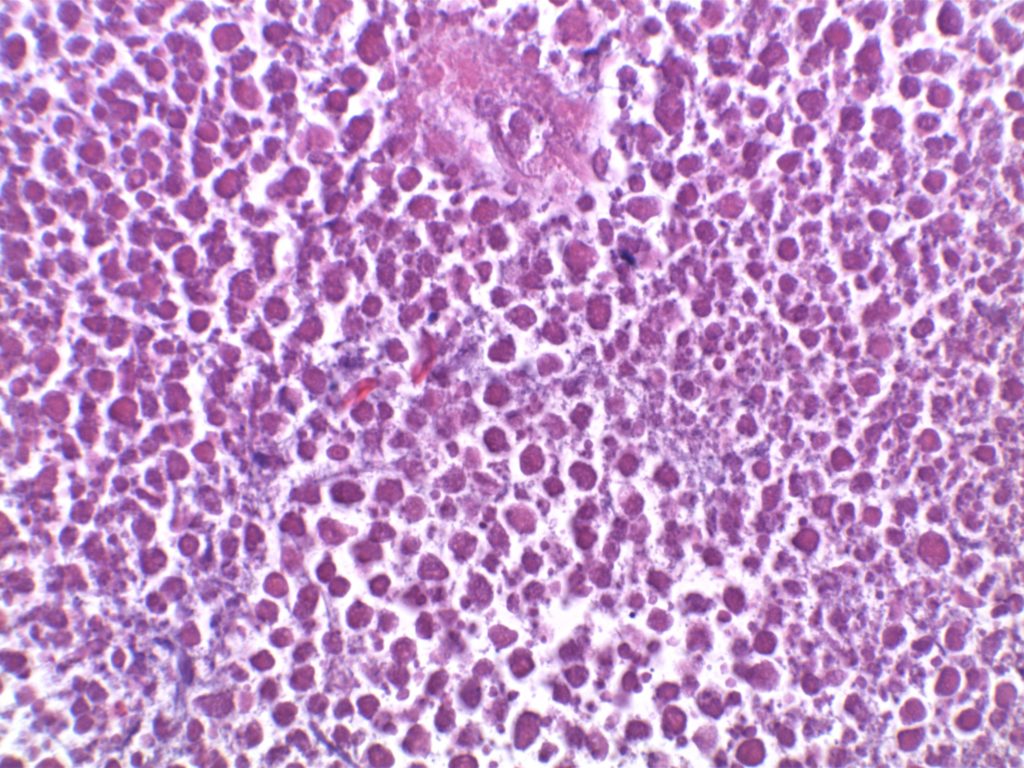
Often, these cases will have extensive necrosis, which may make diagnosis very difficult on small biopsy samples. Additionally, the immunophenotype may vary widely with variable loss and expression of both T and B cell markers.
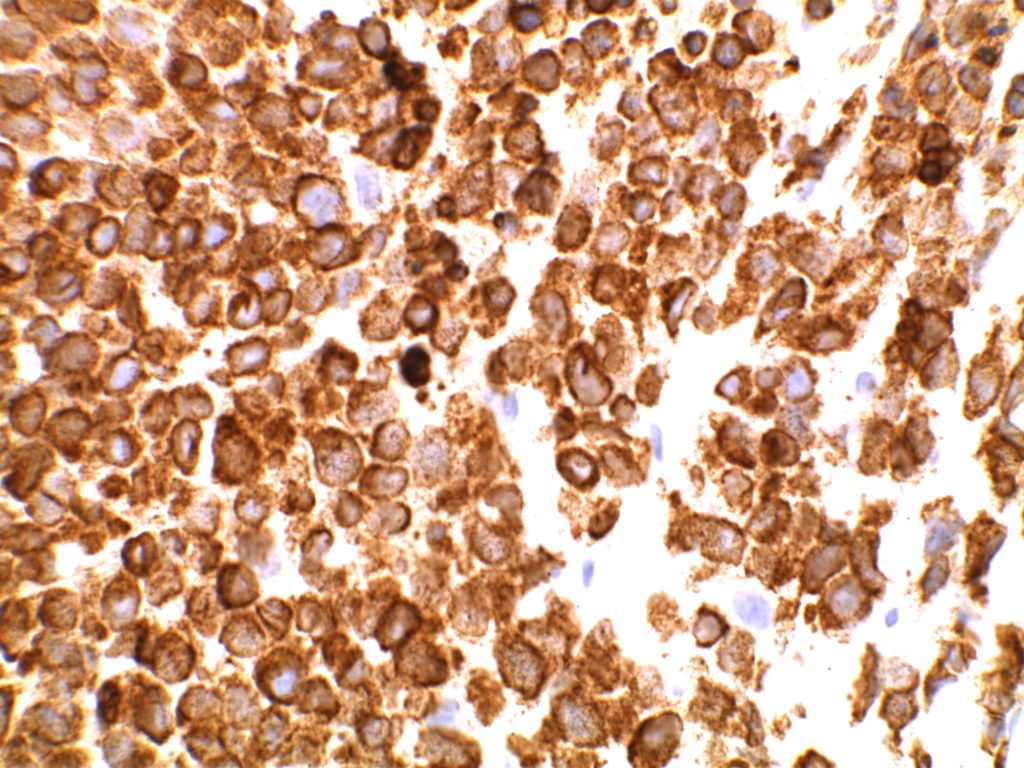
CD20 +
CD79a +
MUM-1 +
CD138 +/-(these cases may be negative for CD20/CD79a)
Subset of cases with T-cell marker expression (CD2, CD3, CD4, and/or CD7)
EBV (EBER) +
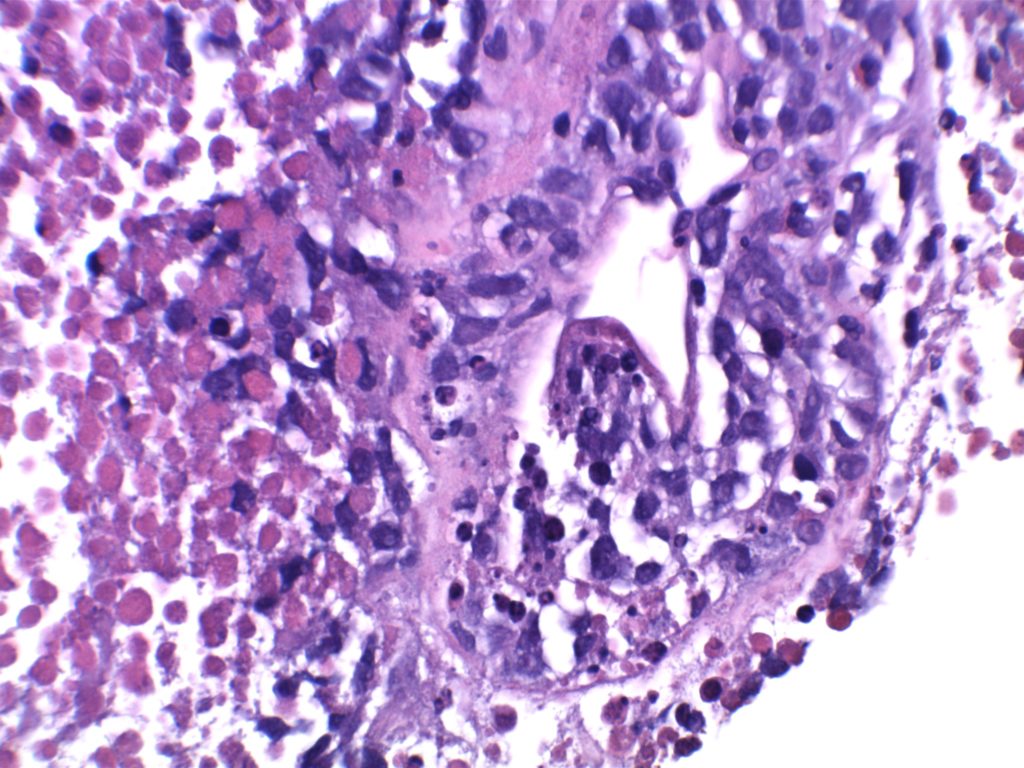
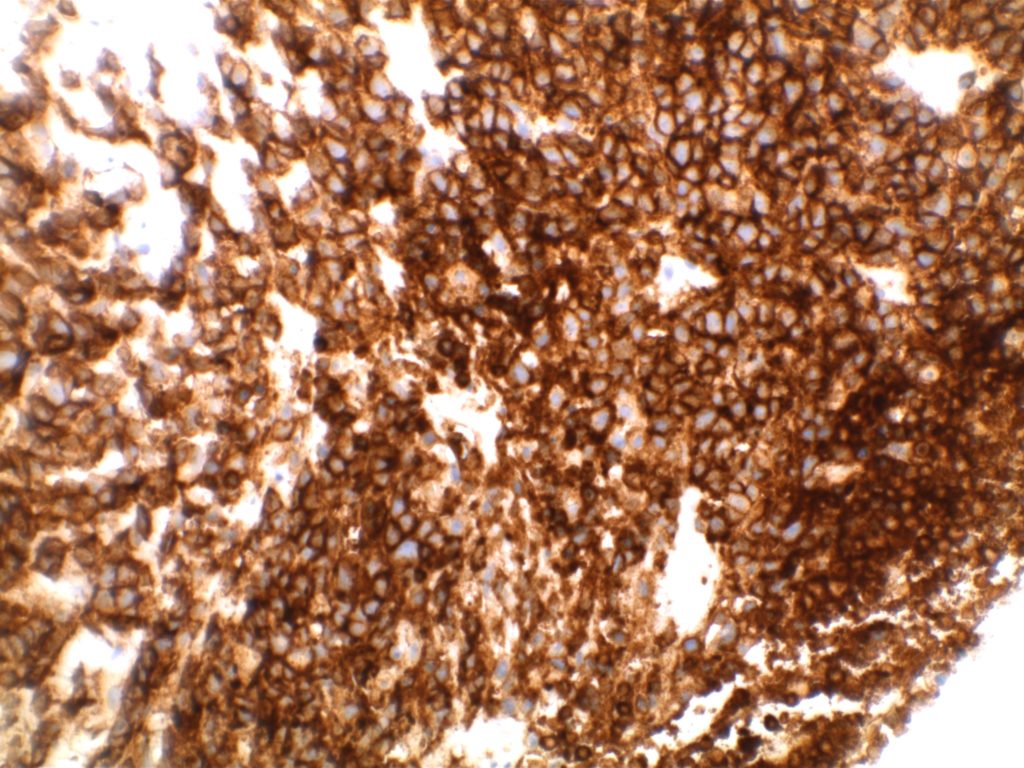
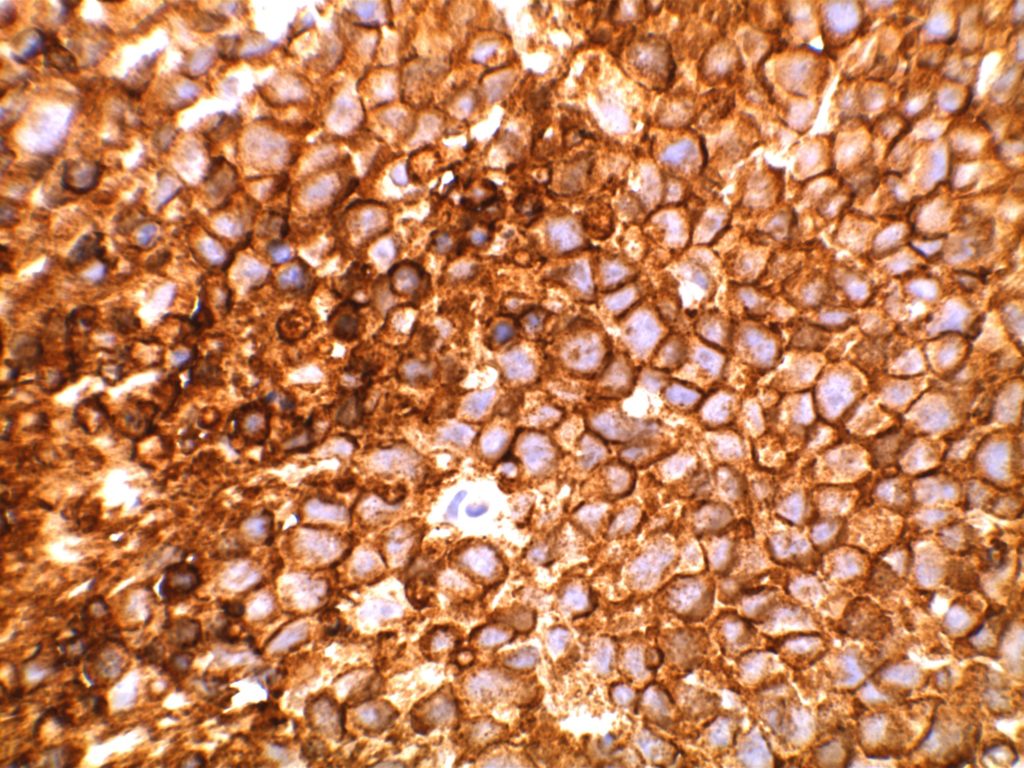
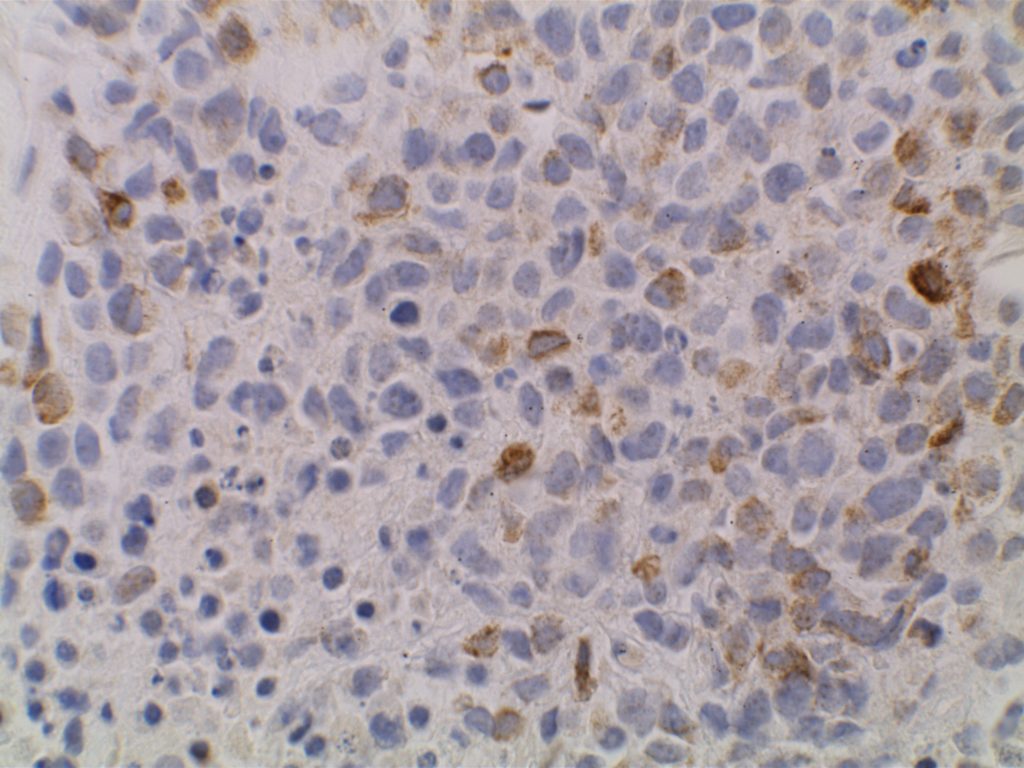
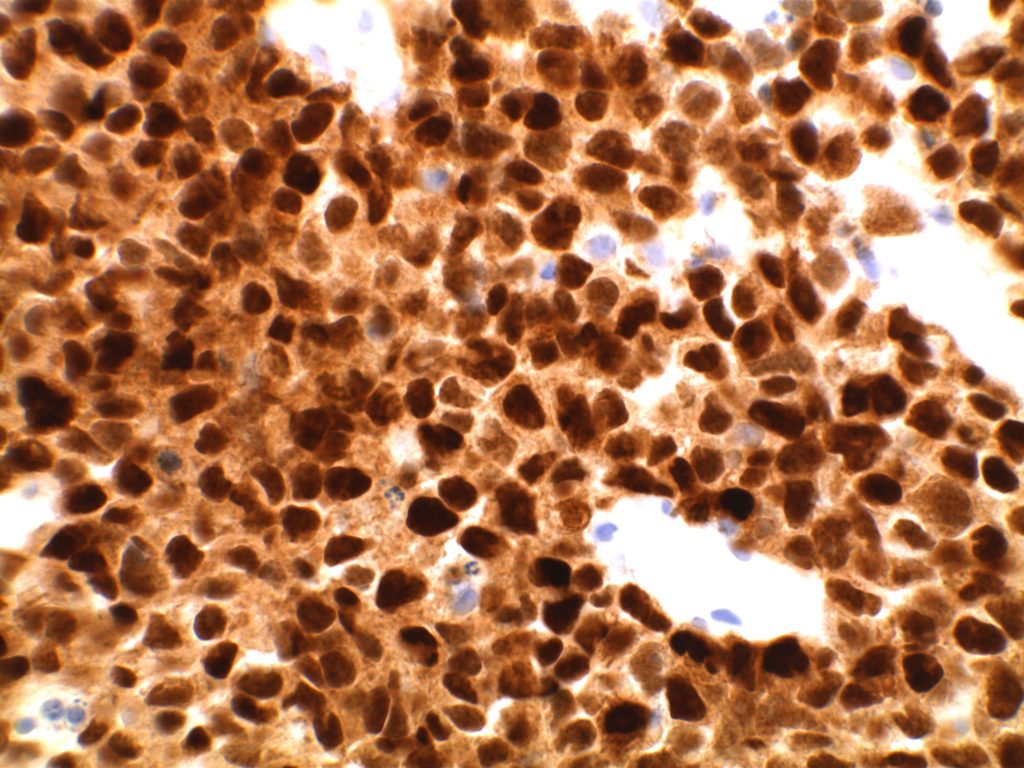
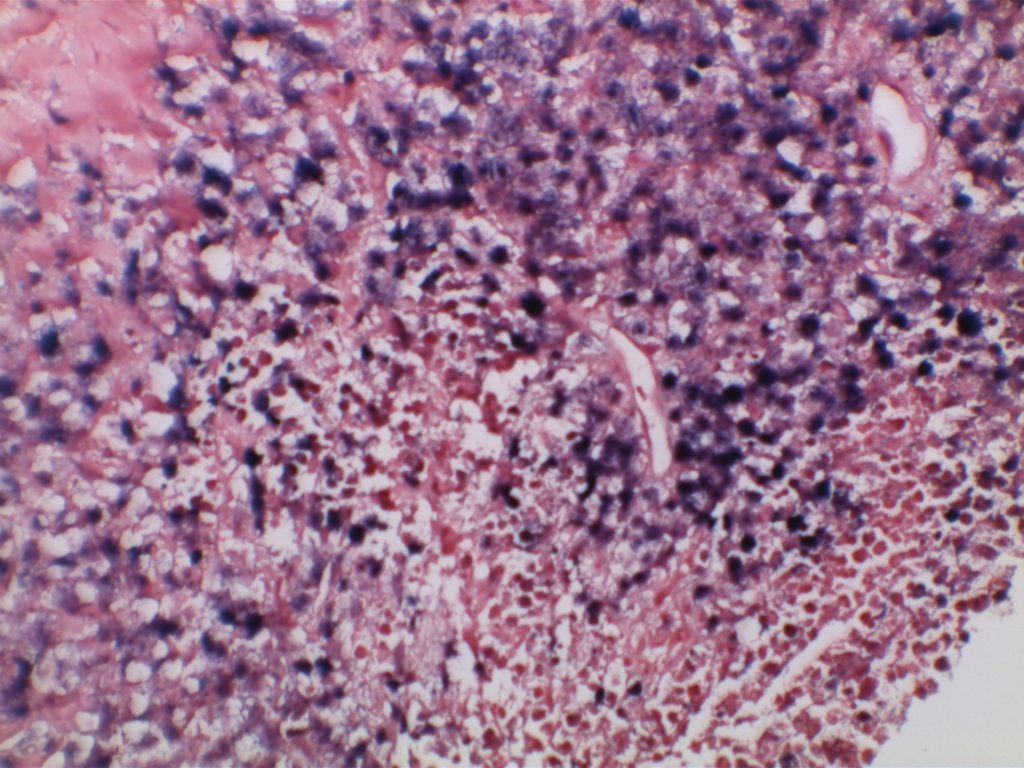
Microscopic images
DLBCL associated with chronic inflammationDLBCL associated with chronic inflammation – Extensive necrosisDLBCL associated with chronic inflammationAberrant CD3 expression in DLBCL associated with chronic inflammationAberrant strong CD7 expression in DLBCL associated with chronic inflammationStrong CD20 expression in DLBCL associated with chronic inflammationDim subset expression of CD79a in DLBCL associated with chronic inflammation.Strong diffuse MUM-1 expression in DLBCL associated with chronic inflammationEBER expression (strong/diffuse) in neoplastic cells of DLBCL associated with chronic inflammation.
References
Loong F, Chan ACL, Ho BCS, Chau Y-P, Lee H-Y, Cheuk W, et al. Diffuse large B-cell lymphoma associated with chronic inflammation as an incidental finding and new clinical scenarios. Mod Pathol. 2010;23: 493–501. doi:10.1038/modpathol.2009.168
Swerdlow SH, Campo E, Harris, NL, Jaffe ES, Pileri SA, Stein H, Thiele J (Eds): WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (Revised 4th edition). IARC: Lyon 2017
The anaplastic variant of diffuse large B-cell lymphoma (DLBCL) is a morphologic variant under the DLBCL, NOS category in the WHO Classification. Typical common features include:
Marked nuclear pleomorphism, often confused with poorly differentiated carcinoma.
Large and significantly enlarged neoplastic cells.
Diffuse Large B-Cell Lymphoma represents a heterogeneous group of non-Hodgkin B-cell lymphoma cases that share a common architectural pattern and large cell size. Subcategorization have been attempted with varying success based on morphology, immunophenotype, and molecular characteristics. Gene expression profiling (GEP) has demonstrated two important groups for both prognosis and treatment. Alizadeh, et al showed significant survival differences in cases of DLBCL with either a germinal center B-cell-like pattern or an activated B-cell-like pattern.
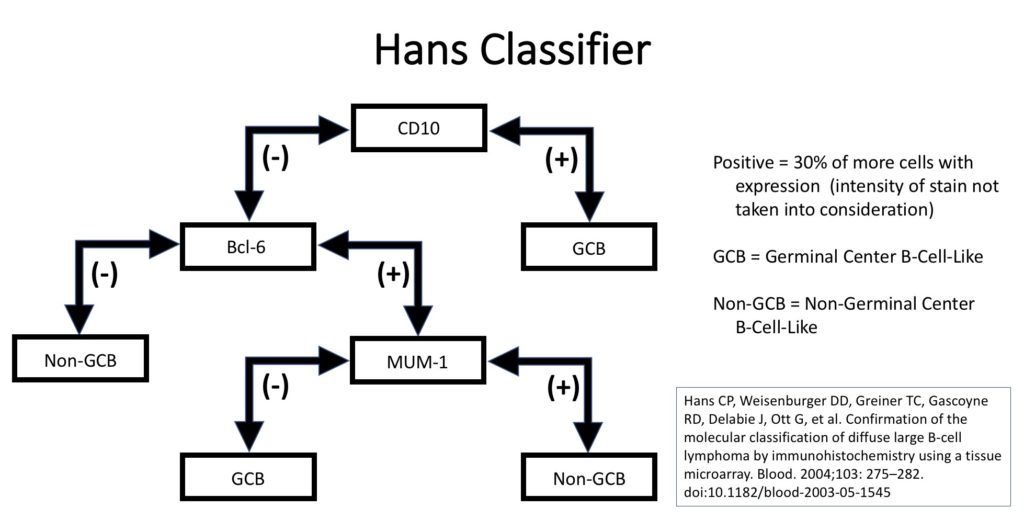
Unfortunately, GEP is not available in routine clinical practice, and multiple surrogate immunohistochemistry (IHC) based algorithms have been developed as a surrogate to GEP. The Hans’ algorithm (classifier) has been one of the most popular methods because it uses only three IHC markers (CD10, Bcl-6, & MUM-1) that are commonly available in most pathology laboratories. The following figure highlights the algorithm for the Hans’ classifier as described in the original paper. The Hans’ algorithm appears to match GEP in 75-80% of cases.
Hans classifier to subtype DLBCL as to germinal center B-cell-like (GCB) or non-germinal center B-cell-like (non-GCB) which has prognostic significance.
Alternative Algorithm(s)
The University of Nebraska group that originally developed the Hans algorithm has developed a new IHC stain algorithm that reportedly classifies cases of DLBCL more accurately compared to the corresponding molecular subtypes (~80% concordance). This algorithm uses GCET1, CD10, BCL-6, MUM-1, and FOXP1 with differing cutoff values for positive/negative. (WW Choi, et al) New algorithms with IHC markers not commonly used in many laboratories has probably limited popularity compared to the Hans’ algorithm. The 2016 WHO hematopathology revision requires that cases of DLBCL be characterized at GCB vs. non-GCB by some acceptable methodology (molecular or IHC).
References
Hans CP, Weisenburger DD, Greiner TC, Gascoyne RD, Delabie J, Ott G, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood. 2004;103: 275–282. doi:10.1182/blood-2003-05-1545
Haarer CF, Roberts RA, Frutiger YM, Grogan TM, Rimsza LM. Immunohistochemical classification of de novo, transformed, and relapsed diffuse large B-cell lymphoma into germinal center B-cell and nongerminal center B-cell subtypes correlates with gene expression profile and patient survival. Arch Pathol Lab Med. 2006;130: 1819–1824.
Chang C-C, McClintock S, Cleveland RP, Trzpuc T, Vesole DH, Logan B, et al. Immunohistochemical expression patterns of germinal center and activation B-cell markers correlate with prognosis in diffuse large B-cell lymphoma. Am J Surg Pathol. 2004;28: 464–470.
Choi WWL, Weisenburger DD, Greiner TC, Piris MA, Banham AH, Delabie J, et al. A new immunostain algorithm classifies diffuse large B-cell lymphoma into molecular subtypes with high accuracy. Clin Cancer Res. 2009;15: 5494–5502. doi:10.1158/1078-0432.CCR-09-0113
Alizadeh AA, Elsen MB, Davis RE, Ma C. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. 2000.
Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127: 2375–2390. doi:10.1182/blood-2016-01-643569
DLBCL is the most common non-Hodgkin lymphoma in the US (25,000 new cases/year) and is an intermediate grade lymphoma consisting of a heterogeneous group of mature B-cell lymphoid neoplasms sharing the common characteristics of diffuse architectural pattern and (medium or large) neoplastic lymphoma cells (nuclei >2x normal lymphocyte or equal to / exceeding a macrophage nuclei). DLBCL lymphoma can arise de novo or as transformation from another lymphoma (e.g. follicular lymphoma, CLL/SLL, marginal zone lymphoma).
CD23 is a transmembrane glycoprotein expressed by different hematopoietic cells and is a low-affinity receptor for IgE. It is also involved in promoting survival of B-cells in the germinal center. CD23 is useful as a follicular cell dendritic cell marker and is classically expressed in cases of CLL/SLL. CD23 has been identified in many types of lymphomas, but is most commonly used to differentiate between CLL/SLL (CD23+) and mantle cell lymphoma (CD23-). This testing is typically performed by flow cytometry, but immunohistochemisty for CD23 is available. Expression of CD23 has been associated with better prognosis (at least in limited published data) in follicular lymphoma, CLL/SLL, mantle cell lymphoma, and diffuse large B-cell lymphoma dependent upon expression characteristics. CD23 is not commonly performed/used as a prognostic marker for B-cell lymphomas.
Rarely CD23 may be expressed in cases of Hairy cell leukemia (17%) and DLBCL (16%). Approximately 70% of Mediastinal large B-cell lymphoma cases express CD23. Practically, this IHC marker is used as a follicular dendritic cell marker and to help differentiate CLL/SLL from mantle cell lymphoma. Follicular dendritic cell tumors will also express CD23 like CD21. CD21 is more sensitive compared to CD23 as a follicular dendritic marker.
Follicular Lymphoma (FL)– CD23 has been found to be expressed in some cases of FL, especially from inguinal lymph nodes, and prognosis appears comparatively better. Olteanuet. al found that 87% of inguinal lymph nodes expressed CD23, compared to 61% from other sites, and that survival was prolonged more in CD23+ cases.
Diffuse Large B-Cell Lymphoma – A subset of DLBCLs may express CD23, which may have a better prognosis (CD23 is not commonly performed for this purpose).
Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma (CLL/SLL)– CD23 expression is characteristic of CLL/SLL, particularly in comparison to another CD5+ lymphoma, mantle cell lymphoma. Strong membrane expression has been associated with a better outcome. DiRaimondo,et. al found ~6% of CLL cases to be CD23 negative (flow cytometry), and they had a worse prognosis. Many of these cases may have been misdiagnosed mantle cell lymphomas.
Mantle Cell Lymphoma (MCL)– CD23 is characteristically negative in MCL, which helps to differentiate it from CLL/SLL. However, ~21% of cases of MCL were found to be CD23+ by Gao,et. al, and other studies have shown CD23 expression in MCL ranging from 0% to 45% (most data appears to be based on flow cytometry).
CD23 Expression Pattern
CLL/SLL – characteristically expressed (6% may be negative, probably much lower)
Mantle cell lymphoma may be CD23+ (21%+, 0-45%)
B-cell Lymphomas (e.g. some DLBCL and follicular lymphomas may show expression)
Follicular Dendritc Cells (not as sensitive as CD21)
B-cells in mantle zone of lymphoid follicles
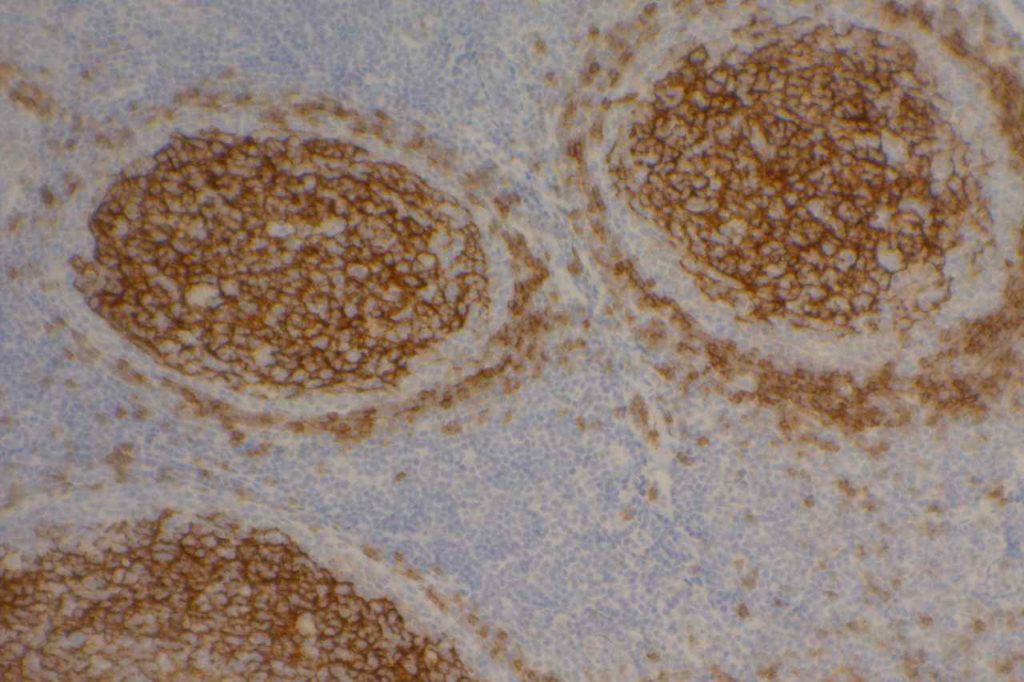
Photomicrographs
CD23 expression highlighting follicular dendritic meshwork in a normal tonsil.
Linderoth J, Jerkeman M, Cavallin-Stahl E, et al. Immunohistochemical expression of CD23 and CD40 may identify prognostically favorable subgroups of diffuse largeB-cell lymphoma: a Nordic Lymphoma Group Study.ClinCancer Res.2003;9:722-728.
Olteanu H, Fenske TS, Harrington AM, Szabo A, He P, Kroft SH. CD23 Expression in Follicular Lymphoma: Clinicopathologic Correlations. Am J Clin Pathol. 2011;135: 46–53. doi:10.1309/AJCP27YWLIQRAJPW
Gao J, Peterson L, Nelson B, Goolsby C, Chen Y-H. Immunophenotypic variations in mantle cell lymphoma. Am J Clin Pathol. 2009;132: 699–706. doi:10.1309/AJCPV8LN5ENMZOVY
Troxell ML, Schwartz EJ, van de Rijn M, Ross DT, Warnke RA, Higgins JP, et al. Follicular dendritic cell immunohistochemical markers in angioimmunoblastic T-cell lymphoma. Appl Immunohistochem Mol Morphol. 2005;13: 297–303.
Dalton RR, Admirand JH, Medeiros LJ. Small Lymphocytic Lymphoma. Pathology Case Reviews. 2004;9: 7.
DiRaimondo F, Albitar M, Huh Y, O’Brien S, Montillo M, Tedeschi A, et al. The clinical and diagnostic relevance of CD23 expression in the chronic lymphoproliferative disease. Cancer. 2002;94: 1721–1730. doi:10.1002/cncr.10401